Last week, the Centers for Medicare and Medicaid Services (CMS) announced that it had approved a reinsurance proposal inWisconsinandMaine in an effort to keep health premiums down. Reinsurance is essentially insurance for insurers: The government helps pay for the cost of exceptionally high-cost claims.
It’s no wonder states have been working on innovative ways to keep premiums affordable for their residents. It seems each day we hear of yet another state announcing double digit premium increases for health insurance:11 percentin Kentucky,19 percentin Washington, and a whopping 24 percent in New York. These are just the proposed rates; increases won’t be made final until immediately before the midterm elections.
Sixty-five percent of Americans reported in a recentReuters/Ipsos pollthat they are “very concerned” about the overall cost of health care — particularly insurance premiums, deductibles, and copays. Rising health care costs affects all Americans: A majority of millennials and baby boomers, whites and minorities, and Democrats and Republicans all reported concerns about increasing costs.
For people who don’t get health insurance from their employers, the cost of health insurance is soaring out of reach. The reason? A relentless campaign by President Trump and Republicans to sabotage the Affordable Care Act (ACA).
President Trump promised Americans cheaper and better health care than what is provided under the Affordable Care Act (ACA). Yet his latest move, to expand access to short-term, limited-duration health plans, may make insurance cheaper but far from better.
These short-term plans have existed under the ACA as a short-term stop-gap measure for people in transition, traveling, or who fall into some gap of ACA coverage (i.e. in states that didn’t expand Medicaid). But now, the Trump administration wants to treat these plans, which are exempt from ACA rules and protections, as long-term solutions that will be renewable for up to three years. These plans can charge more for people with preexisting conditions, deny coverage of certain essential health benefits and have annual caps on coverage.
We all want cheap health insurance – until we get sick. Then we want our health plan to pay for the care we need to get well again. These plans are cheaper, until you need them. Then you’ll be on the hook for your health care costs.
The Kaiser Family Foundation found that of short-term plans currently on the market, 71 percent did not cover outpatient prescription drugs, 62 percent did not cover mental health services, and no plan covered maternity care. Of the plans that covered these services, most had strict benefit limits, such as a $3,000 limit on prescription drug coverage.
Insurance plans with skimpy benefits were what led to the ACA. So many consumers were left with limited coverage when they got sick or were denied coverage because of a preexisting illness. Congress passed the ACA to regulate the market and mandate that products sold as ‘insurance’ meet certain requirements – such as the covering of essential health benefits and not charging more for preexisting conditions.
And voters continue to support protections for preexisting conditions. A Kaiser Health Tracking Poll found that “a candidate’s position on continuing protections for people with pre-existing health conditions is the top health care campaign issue for voters, among a list of issues provided.” Support for these protections cuts across demographics: most Democratic voters (74 percent), independent voters (64 percent), and voters living in battleground areas (61 percent) said that a candidate’s position on protections for preexisting conditions “is either the single most important factor or a very important factor in their 2018 vote.” Roughly half of Republican voters reported the same.
Unfortunately, what is likely to happen when these products are treated as regular plans, is that healthy people ineligible for subsidies will take the risk that they won’t get sick and need comprehensive coverage. Pulling this population out of the ACA individual market means that only people eligible for subsidies and the sicker people that need comprehensive coverage will stay. This drives up costs for the population already most vulnerable in the changing individual market: people with preexisting conditions and ineligible for subsidies.
It is true that protections for people with preexisting conditions contributed to increased costs in the individual market, but there are other policies – such as increasing subsidies, passing a comprehensive reinsurance program, expanding Medicaid in all states, and curbing cost growth – that could help bring down costs.
Allowing insurers to sell stop-gap short-term insurance that doesn’t cover consumers when needed is a bad way to reduce health care costs. For those who never get sick, it could work. But if anyone gets an unfortunate diagnosis, gets pregnant, or breaks a bone in a sporting event, they may not be covered. And paying for your care out of pocket is, after spending hundreds of dollars on insurance, never cheap.
Americans who buy health insurance on the exchanges set up by the Affordable Care Act (ACA) are having sticker shock as preliminary rates are filed for the 2019 plan year. Healthcare analysts expect insurance premiums to skyrocket during the next open enrollment period, which inconveniently begins just before the 2018 midterm elections. These higher premiums will be the direct result of changes in the ACA pushed through Congress by the
Trump administration and Republicans – changes explicitly intended to sabotage the ACA (“Obamacare”) by destabilizing healthcare markets. A bipartisan solution, reinsurance, is needed to undo the damage inflicted on the individual market.
Several times in the past, I’ve examined the contribution of pharmaceuticals to rising health care costs (here, here, and here). It seems appropriate to do again, given President Trump’s latest tweets on drug prices, and Pfizer’s decision to roll back recent price hikes.
I note first that an April 2018 report from the IQVIA Institute entitled Medicine Use and Spending in the U.S. found that net spending on medicines (including both generics and branded products, and both retail and institutional use) rose by only $1 billion in 2017, or 0.6%. By contrast total personal healthcare spending is projected to have risen by $124 billion, or 4.4% in 2017. That means there is no sign of out-of-control drug spending in 2017.
In the first five months of 2018, the average price of prescription drugs rose by 2.5%, according to data from the Bureau of Labor Statistics. That’s almost identical to the overall consumer price inflation of 2.4%. So there’s no sign from the BLS data of excess drug price increases in 2018.
Finally, we do a five year look-back (2012-2017), which includes the high cost years of 2014 and 2015. We find that net spending on medicines rose by $68 billion over that stretch, or 26.7%. By comparison, total personal health care spending rose by $591 billion over that stretch, or 25.0%. In other words, generic and branded medicines only contributed 12% of the increase in personal health care spending between 2012 and 2017. Net spending on medicines rose at roughly the same rate as all other healthcare costs.
Another useful comparison: Between 2012 and 2017, health care labor costs rose by an estimated $231 billion, contributing almost 40% of the increase in personal healthcare spending. These are mostly propelled by the rapid increase in the healthcare workforce, which has increased by 1.4 million since 2012 alone.
All told, policy makers who are concerned about healthcare costs would be better off focusing on restraining the runaway growth of healthcare workers.
President Trump’s nomination of Judge Brett Kavanaugh to fill the seat on the Supreme Court vacated by Justice Anthony Kennedy have left many to wonder: What will replacing an often swing vote with a more conservative one mean for health care? There are many pending cases in lower courts that, if they make it a more conservative Supreme Court, could define health policy for years to come.
Preexisting conditions
Nineteen conservative states, led by the Texas attorney general, are seeking to overturn the Affordable Care Act. The U.S. Department of Justice announced that it would not defend the law in court. The agency argued that with the abolishment of the individual mandate penalty in 2019, community rating and guaranteed issue — the rules that protect those with preexisting conditions — are unconstitutional. If the case makes it to the Supreme Court, the newest member could be a deciding vote on whether or not preexisting condition protections should continue.
Abortion
Though a recent poll found that both men and women support by a two-to-one margin Roe v. Wade, which struck down state laws restricting access to abortion, a number of abortion-related cases are working their way through lower courts. They directly ask critical questions, from at how many weeks abortion should be allowed to what type of facilities and providers can terminate a pregnancy. These cases could all be opportunities for the high court to preserve or limit access to abortion in the United States.
Two weeks ago, the U.S. Department of Justice (DOJ)filed a legal brief in support of a Texas lawsuit that would kill one of themost popular provisionsof the Affordable Care Act (ACA): the one that ensures people with past medical problems can get affordable health insurance. It’s the latest twist in the Trump administration’s unrelenting campaign to sabotage “Obamacare,” even if that means pricing sick Americans out of health coverage altogether.
The DOJ’s intervention raised eyebrows since it marked a further politicization of a federal agency whose mission is to enforce laws passed by Congress. Instead, it is trying to unravel the law that President Trump and his party failed repeatedly to “repeal and replace.” It’s an undemocratic run around the legislative branch, an attempt by President Trump to win in court what he could not win in Congress.
Generally speaking, if you have a preexisting condition — a chronic condition such as asthma, a past cancer diagnosis, or pregnancy — and are covered by Medicare, Medicaid, or private group insurance, you are protected financially from the costs of those conditions. But prior to the ACA, those in the individual, or non-group, market could be denied coverage for being sick or pregnant. In fact, 18 percent of individual market applicantswere deniedcoverage before the ACA and many more did not apply for coverage or were offered it only at unaffordable prices. Today, roughly 27 percent of adults(52 million people)not eligible for Medicare have preexisting conditions — these people would be the most at risk if these protections are thrown out.
It’s no secret that the American health care system is far from perfect. The United States spends a higher percentage of our gross domestic product on health care thanany other countrydespite having comparable outcomes. And although the Affordable Care Act successfully reduced the percentage of uninsured Americans by almost half between2010and 2016,8.8 percentstill had no coverage according to the most recent Census estimate – one of thehighest rates of any OECD country. Moreover, Republican sabotage of the ACA has threatened to dramaticallyincrease costsandreversemuch of these coverage gains.
Many Democrats have embraced “Medicare for All” as their preferred mechanism for addressing these problems. Medicare is already one of the largest health insurers in the United States, covering about one sixth of the population, including most Americans over the age of 65, as well as a select few other groups, such as individuals with disabilities. Expanding Medicare to cover the rest of the population has a natural appeal given the program’s overwhelming popularitywith both beneficiaries and the general public. But this week’s report from the program’s trustees warns of serious financial challenges that threaten Medicare’s ability to meet its obligations to current beneficiaries. The program cannot be expanded unless these problems are resolved and benefits can be sustainably financed.
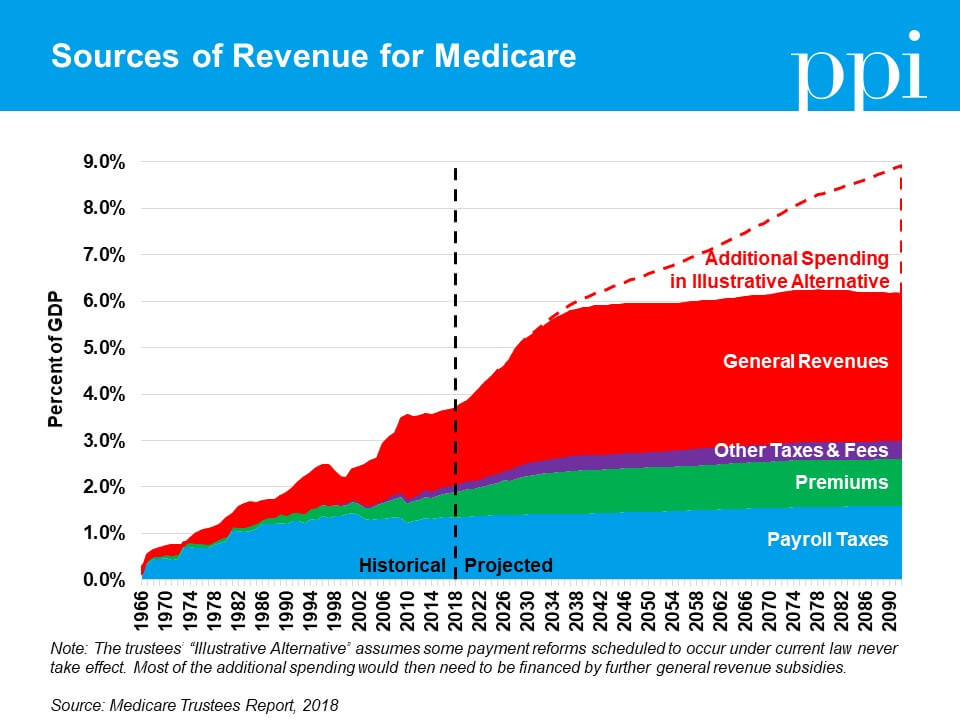
Medicare consists of two financing mechanisms: Hospital Insurance (HI) and Supplemental Medical Insurance (SMI) trust funds. The HI trust fund pays for Medicare Part A, which covers hospital services, nursing facilities, home health assistance, and hospice care. HI is primarily funded by premiums and a payroll tax of 1.45 percent paid by both workers and their employers (or 2.9 percent in the case of self-employed workers who are required to pay both taxes). In years when these revenue sources exceed spending, the Treasury Department credits the HI trust fund for the balance. In subsequent years when spending exceeds revenue, Medicare can then draw upon these surpluses to make up the shortfall.
Although HI used to have regular annual budget surpluses up until 2004, it is now runningchronic cash deficits. The trustees report projects that the trust fund will be exhausted by 2026, at which point Medicare would only have enough revenue to meet91 percentof its Part A obligations. The HI trust fund’s exhaustion date is typically the metric most commonly cited in the media when discussing Medicare’s financial health, but in reality it’s only the tip of the iceberg: the challenges facing HI pale in comparison to those facing SMI.
Unlike HI, SMI – which covers both Medicare Part B (outpatient services and medical equipment) and Part D (prescription drugs) – only receives about one quarter of its revenues from dedicated sources. The remainder is automatically funded by general revenues, which ensures that SMI can never become insolvent but also obscures the true cost to both voters and policymakers. This structure is particularly problematic because Medicare is the fastest growing program in the federal budget: as the total size of SMI grows, it threatens tocrowd out other public prioritiesthat compete for the same pool of resources even if the proportion of the program funded by general revenues remains the same.
When taken together, Medicare’s dedicated revenue sources only cover about half of its spending. In that context, it makes sense that many voters would feel they get a better deal out of Medicare than other forms of insurance – they’re only seeing half the cost. Additionally, there are far more workers paying taxes into Medicare than there are beneficiaries. The Medicare model works for providing subsidized care to targeted subsets of the population, but if it were extended to cover the whole population, suddenly there would be fewer taxpayers than beneficiaries and no way to defray the cost.
One alternative that several moderate Democrats have suggested is to offer consumers an option to buy into Medicare voluntarily instead of automatically enrolling the entire population. This “public option” approach would preserve the private health insurance market but allow a public plan to compete. If the public plan is able to deliver more efficient health services or achieve lower prices through the use of Medicare’s rate-setting system, it could eventually grow to dominate the market through consumer choice and develop into a de facto single-payer system.
Before policymakers go this route, however, they need to ensure that any public option is self-financed through premiums (asmany of the current proposalsrecommend). To the extent coverage is subsidized by the government, it must be limited to the same subsidies consumers receive from programs such as those in the Affordable Care Act to purchase private insurance. Should the public option be subsidized by general revenues the same way as SMI, it would become increasingly unsustainable as market share grows – an outcome would be bad for taxpayers and beneficiaries alike.
Lynnel Beauchesne’s dental office hugs a rural crossroads near Tunnelton, W.Va., population 336. Acres of empty farmland surround the weathered one-story white building; a couple of houses and a few barns are the only neighbors. But the parking lot is full. Some people have driven hours to see Beauchesne, the sole dentist within 30 miles. She estimates that she has as many as 8,000 patients. Before the office closes at 7 p.m., she and her two hygienists will see up to 50 of them, not counting emergencies.
About 43 percent of rural Americans lack access to dental care, according to the National Rural Health Association, and West Virginia, among the poorest and most rural states, is at the center of the crisis. All but six of the state’s 55 counties include federally designated “Health Professional Shortage Areas,” “Medically Underserved Areas” or both. The state’s Oral Health Program found in 2014 and 2015 that nearly half of counties had fewer than six practicing dentists, just half of adult West Virginians had visited a dentist in the previous year, and more than one-fifth hadn’t seen a dentist in five years. By comparison, a U.S. Centers for Disease Control and Prevention study in 2015 found that 64 percent of all American adults ages 18 to 64 reported seeing a dentist in the previous year. The rate of total tooth loss is 33.8 percent among West Virginians over 65, compared with roughly 19 percent for all seniors nationally.
One seemingly obvious solution is to persuade more dentists and other oral-health providers to come to places like West Virginia, a goal of various public efforts. The federal National Health Service Corps program, for example, offers up to $50,000 in loan assistance to doctors and dentists willing to work two years in a designated shortage area. And several states have passed or considered legislation authorizing “dental therapists” — midlevel providers akin to nurse practitioners — to provide certain kinds of primary dental care in areas where dentists are scarce.
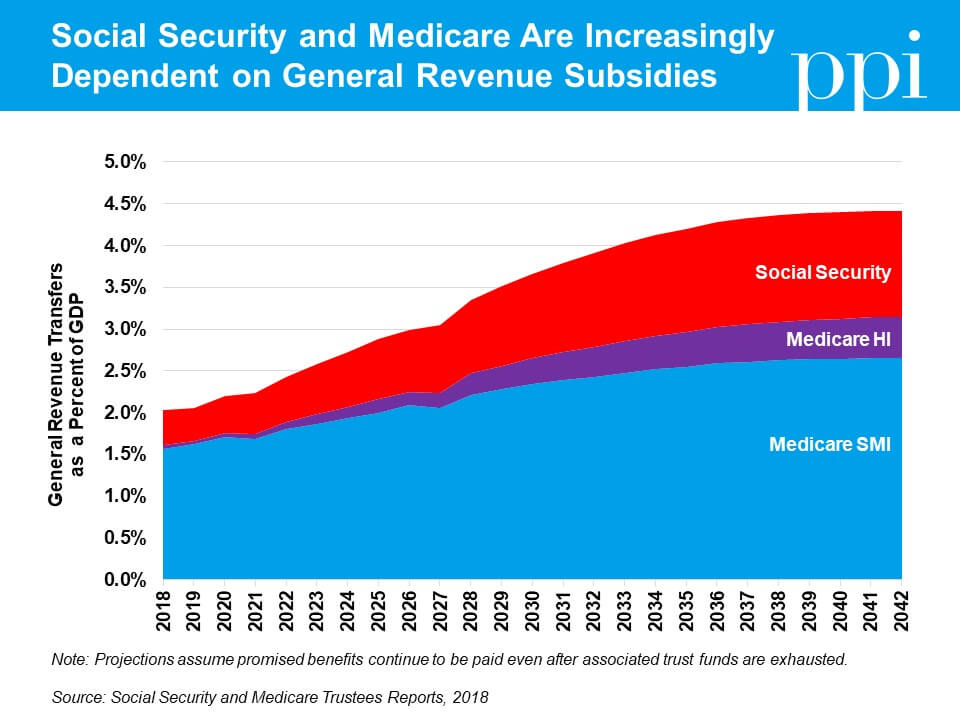
The new reports released yesterday by the trustees forSocial SecurityandMedicarewarn that both programs face a growing gap between scheduled benefits and the dedicated revenue sources that finance them. If nothing is done to address the shortfalls in these programs, they will pose a grave threat to both the beneficiaries who depend on Social Security and Medicare and the other critical public investments that will increasingly have to compete with these programs for limited resources.
Unlike most programs in the federal budget, which are funded from the same pool of general revenues, Social Security and Medicare were designed with dedicated revenue sources intended to finance their benefits (primarily payroll taxes for Social Security and a combination of taxes, premiums, and fees for Medicare). But in 2017, Medicare required $307 billion in general revenue funding to meet its obligations, while Social Security required another $41 billion – a combined gap which equaled roughly two percent of gross domestic product.
In less than 20 years, that gap will double to more than four percent of GDP as the baby boomers move into retirement and theratio of workers to beneficiariesfalls. This growth places an enormous burden on the rest of the federal budget by increasingexisting deficitsand creating competition with all the other federal programs, from defense to education, that require general revenue funding. For comparison,discretionary spending– the part of the budget that includes all federal spending appropriated annually by Congress, including everything from the military to infrastructure funding – totaled just 6.3 percent of GDP in 2017 and is set to fall in future years.
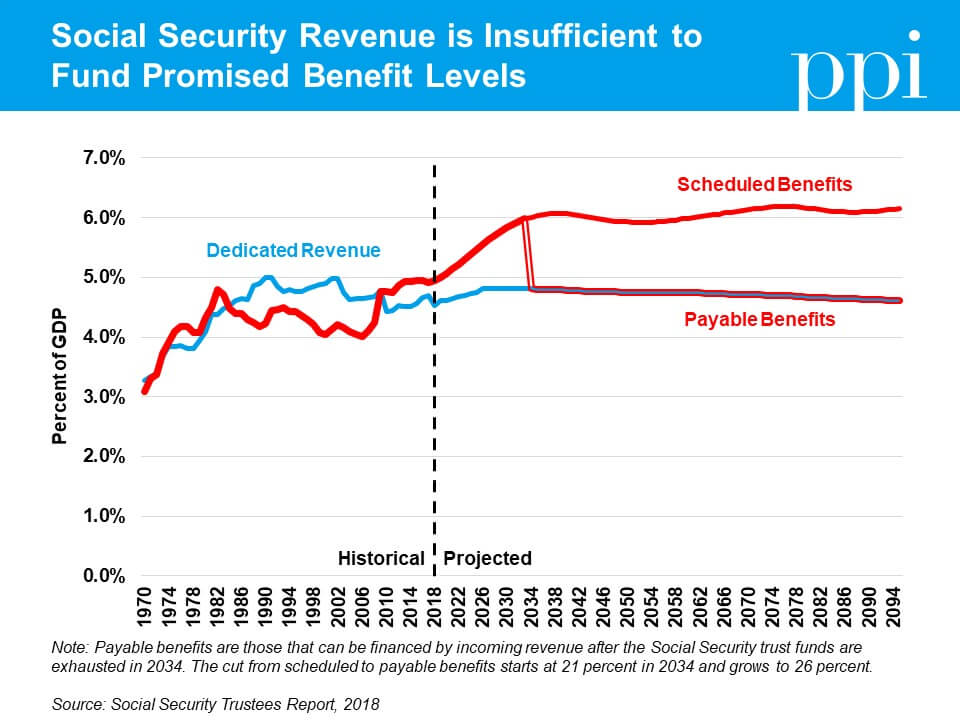
Under current law, Social Security and Medicare are allowed to spend more than they collect in dedicated revenue, but only up to a point. In years when dedicated revenue exceeds spending, the Treasury Department credits one of four trust funds for the balance: the Old Age and Survivors Insurance (OASI) and Disability Insurance (DI) trust funds for Social Security, and the Hospital Insurance (HI) and Supplemental Medical Insurance (SMI) trust funds for Medicare. In subsequent years when spending exceeds revenue, Social Security and Medicare can then use transfers from general revenue to draw upon these established surpluses and make up their annual shortfall.
Once the fund balances are exhausted, however, benefits are automatically reduced to what is payable with incoming revenue (except for SMI, which by design is partially funded with general revenues and can never be exhausted). The trustees projected the following trust fund exhaustions in their reports:
HI will be exhausted in 2026, at which point benefits would be reduced by 9 percent;
DI will be exhausted in 2032, at which point benefits would be reduced by 4 percent;
OASI will be exhausted in 2034, at which point benefits would be reduced by 23 percent; and
If OASI and DI were combined, they would be exhausted in 2034, at which point benefits would be reduced by 21 percent – a cut that would gradually increase to 26 percent as the gap between revenues and scheduled benefits continues to grow.
Waiting until the last minute to address these shortfalls would be catastrophic for a number of reasons. First, it creates the prospect of sudden and draconian benefit cuts for seniors and individuals with disabilities. Uncertainty about the future of Social Security and Medicare undermines the ability of all Americans to plan for their retirement accordingly and risks jeopardizing public support for the program. In fact, recent polls have found a majority of Americans bothyoungandoldalready lack confidence in the ability of Social Security and Medicare to pay future benefits as scheduled. Restoring long-term solvency to these programs would help restore public confidence in them as well.
The alternative to sudden benefit cuts, that future workers will be asked to bear the entire cost of poor decisions made by previous generations, is hardly better. The Social Security trustees note in their report that if action were delayed until 2034, policymakers would need to immediately and permanently increase revenue by an amount equal to a one-third increase in the payroll tax rate to prevent sudden benefit cuts in Social Security alone. Combined with the even-larger tax increases necessary to fully fund Medicare, this would be an enormous tax burden to place entirely on the shoulders of tomorrow’s workers. The longer policymakers wait to begin phasing in changes, the harder it will be to have older generations contribute to the solution and defray the burden.
Finally, the competition for limited resources created by growing general revenue subsidies threatens to crowd out other important progressive priorities. General revenue isalready insufficientto cover current spending levels – a reality that pre-dated last year’stax legislation. Because the trust funds aren’t invested as external savings, the government must borrow from private investors to repay the trust fund surpluses as they’re drawn down (replacing this intragovernmental debt with more economically significant debt held by the public). This debt comes with added interest costs, further increasing the pressure on the federal budget.
In the coming years before trust fund exhaustion, funding that could be used for public investments in our future such as infrastructure, education, and scientific research will be increasingly consumed by growing subsidies for social insurance programs and interest costs. Even worse would be a scenario in which policymakers use the existence of the trust funds as an excuse to delay action on correcting the imbalances between dedicated revenues and spending, only to abandon the system and provide unlimited infusions of general revenues when the trust funds’ exhaustion would otherwise force hard choices.
We can do better. Our elected officials shouldtable costly policy proposalsthat threaten to make the problem worse and instead work towards phasing in pragmatic reforms to strengthen and secure the future of these important programs.
In the future, medicine will be tailored to your individual “genome” or genetic code, lifestyle and community. Rather than a one-size-fits-most treatment, doctors will use data to determine what therapies you should receive based on genetic traits you’ve inherited from family, your daily habits, and where you live.
But how do we get there?
We need to understand how a person’s genome impacts their health outcomes. Everyone has a completely unique genome — the 3 million DNA pairs that determine their physical selves. This code influences your risk factors for inherited conditions and how you might respond to medication.
Federal policy should move beyond fee-for-service and prioritize prevention
Nearly half a million Americans suffering from kidney failure depend for their survival on dialysis.For many of them, life is nasty, brutish, and short.
One in four dialysis patients will die within the first year of treatment, and six in 10 will die within five years.Patients typically spend four hours a day, three days a week, tethered to the machines that draw out their blood, filter it, and return it to them. Chills, fever, and crippling fatigue are common – as are heart attacks, due to the stress of pumping patients’ blood through the machines at the rate of a pint per minute.Infections are commonplace too, particularly for patients outfitted with chest catheters, nicknamed the “great white tubes of death” because of their ability to send pathogens straight into a patient’s heart and bloodstream.
Under Gov. Gina Raimondo, Rhode Island is aiming to rebuild its economy — once factory-based — around advanced industries such as biotech and software. With such projects as the Providence Innovation & Design District, the goal is to create good-paying jobs by attracting leading-edge companies to the state.
How odd, then, that the state legislature is considering a bill that would block an important health care innovation that would not only lower costs, but improve care as well. Senate Bill 2404 would dramatically restrict the use of online vision tests, an emerging telemedicine technology that is in use today. That’s bad news for Rhode Island.
In October 2017, Governor Jerry Brown of California signed a “drug price transparency bill,” requiring pharma and biotech companies to give advance notification of significant price increases and provide specific justifications. Brown hailed the bill as a big step toward holding down spending on health care. “Californians have a right to know why their medical costs are out of control,” said Brown.
Many other states are finding the pharma industry to be a tempting target, especially with all the media attention given to a small number of high-profile price hikes. In Maryland, a new “price-gouging” law restricts generic and off-patent medicines from “excessive and not justified” price increases. Nevada has tackled the cost of diabetes medicines such as insulin, requiring drug makers that have raised list prices by a significant amount to release data about the costs of making and marketing the drugs. Other states like New York, New Hampshire, and Maine are considering legislation that would take various approaches to controlling drug pricing as a solution to rising health care costs.
But a new study by the Progressive Policy Institute suggests that state-level drug price laws potentially harm competition and boost drug costs, while doing very little to slow down the overall growth of health care costs. First, we describe the range of state-level drug price laws – both the ones that have been enacted and the ones that are under consideration.
Healthcare faces three major issues: access, cost, and productivity. Telemedicine — the use of technology to help treat patients remotely – can help address all three. Broadband allows many underserved rural and minority communities that previously had limited access to medical services to remotely access high-quality medical care. Telemedicine reduces the need for expensive real estate and enables providers to better leverage their current medical personnel to provide improved care to more people.
But, despite its benefits, there is an ongoing struggle about how to regulate telemedicine: who can practice it, what services can be delivered via telemedicine, and how it should be reimbursed. As is the case with any innovation, policymakers are looking to find the right balance between encouraging new technologies and protecting the health of patients. These are real issues. In too many cases, however, state and local legislators have erred on the side of too many restrictions on telemedicine, driving up prices and “protecting” patients from cheaper, better care.
In particular, online vision tests have come under attack in some states. Online vision tests use your computer and smartphone to assess your near and distance vision. When used correctly, they complement rather than substitute for in-person eye exams. Their main benefit is that they make it easier and less costly to get prescriptions for glasses or contacts. That’s especially helpful in states with large rural or poor urban communities. Indeed, more than 800 counties nationally have no optometrist offices or optical goods stores, according to figures from the Bureau of Labor Statistics. That’s fully one-quarter of the counties in the country.
In this report, we provide background on the health and economic benefits of telemedicine, analyze recent legislation proposed regarding online vision tests, and illustrate the impact online vision tests have on poor and rural communities.
It’s been a surreal political year, but PPI has much to celebrate this holiday season. Throughout 2017, we expanded our productive capacity and the scope of our political and media outreach significantly. For example, PPI organized 150 meetings with prominent elected officials; visited 10 state capitals and 10 foreign capitals, published an influential book and more than 40 original research papers, and hosted nearly 30 private salon dinners on a variety of topical issues.
Best of all, we saw PPI’s research, analysis, and innovative ideas breaking through the political static and changing the way people think about some critical issues, including how to revive U.S. economic dynamism, spread innovation and jobs to people and places left behind by economic growth, and modernize the ways we prepare young people for work and citizenship.
Let me give you some highlights:
This fall, David Osborne’s new book, Reinventing America’s Schools, was published on the 25th anniversary of the nation’s first charter school in Minnesota. David, who heads PPI’s Reinventing America’s Schools project, documents the emergence of a new “21st Century” model for organizing and modernizing our public school system around the principles of school autonomy, accountability, choice, and diversity. David is just winding up a remarkable 20-city book tour that drew wide attention from education, political, and civic leaders, as well as the media. Because David is a great storyteller, as well as analyst, it’s a highly readable book that offers a cogent picture of a K-12 school system geared to the demands of the knowledge economy. It makes a great holiday gift!
Dr. Michael Mandel’s pioneering research on e-commerce and job creation also upended conventional wisdom and caught the attention of top economic commentators. Dr. Mandel, PPI’s chief economic strategist, found that online commerce has actually created more jobs in retail than it destroys, and that these new jobs (many in fulfillment centers in outlying areas) pay considerably better than traditional ones. His research buttresses the main premise of PPI’s progressive pro-growth agenda: that spreading digital innovation to the physical economy will create new jobs and businesses, raise labor productivity, and reduce inequality.
PPI challenged the dubious panacea of “free college” and proposed a progressive alternative – a robust system of post-secondary learning and credentials for the roughly 70 percent of young Americans who don’t get college degrees. PPI Senior Fellow Harry Holzer developed a creative menu of ways to create more “hybrid learning” opportunities combining work-based and classroom instruction. And PPI Senior Fellow Anne Kim highlighted the inequity of current government policies that subsidize college-bound youth (e.g., Pell Grants), but provide no help for people earning credentials certifying skills that employers value.
Building on last year’s opening of a PPI office in Brussels, we expanded our overseas work considerably in 2017. In January, I endeavored to explain the outcome of the U.S. election to shell-shocked audiences in London, Brussels, and Berlin. In April, we led our annual Congressional senior staff delegation to Paris, Brussels, and Berlin to engage European policymakers on the French presidential election and other U.S-E.U. issues, including international taxation, competition policy, and trade. PPI also took its message of data-driven innovation and growth to Australia, Brazil, Japan and a number of other countries.
Other 2017 highlights included a strategy retreat in February with two dozen top elected leaders to explore ideas for a new, radically pragmatic agenda for progressives; a Washington conference with our longtime friend Janet Napolitano (now President of the University of California system) on how to update and preserve NAFTA; public forums in Washington on pricing carbon, infrastructure, tax reform, and other pressing issues; creative policy reports on varied subjects; and a robust output of articles, op-eds, blogs, and social media activity.
I’m also happy to report many terrific additions to PPI in 2017. Rob Keast joined to manage our external relations and new policy development; Paul Bledsoe assumed a new role as Strategic Adviser as well as guiding our work on energy and climate policy; and Emily Langhorne joined as Education Policy Analyst. We will also be adding a fiscal project next year.
All this leaves us poised for a high-impact year in 2018. In this midterm-election year, our top priority will be crafting and building support for a new progressive platform — a radically pragmatic alternative to the political tribalism throttling America’s progress. That starts with new and better ideas for solving peoples’ problems that look forward, not backward, and that speak to their hopes and aspirations, not their anger and mistrust.
It’s a tall order, and we cannot succeed without your help and support. Thanks for all you have done over past years, and we look forward to working with you in 2018.
Innovation is the foundation of growth. As innovation spreads to the physical industries, the result is higher wages, lower costs, and a more dynamic economy, as we showed in our recent report, The Coming Productivity Boom.
But innovation in physical industries has proceeded slower than we might have wanted, In part, that’s because promising technologies are being hindered at the state and local level. Consider the humble eye refraction. Some companies are rolling out technologies that enable ordinary people to do eye refractions remotely, using computers or smartphones. Such a technology has the potential to greatly reduce the cost of updating and renewing contact lens prescriptions, while enabling people to check their eyes more often.
Unfortunately, in Connecticut, the state legislature is now considering a bill that would undercut the use of remote eye refractions. The bill says, in part:
No provider shall issue an initial prescription to or renew an initial prescription for a patient without having performed an in-person evaluation and an eye examination of the patient.
In other words, everyone has to make an expensive and time-consuming in-person trip to an eye doctor to get a prescription renewal for contact lens, even if the remote refraction says no change. This requirement could be especially costly in Connecticut, where optometrists make $192,870 per year on average, the highest in the country, according to the Bureau of Labor Statistics.* Indeed, Connecticut is the only state where optometrists make more than family and general practitioners, based on BLS data.
Remote refraction can and should never replace in-person visits to optometrists and ophthalmologists. But in a world where health care costs are increasingly squeezed, it seems silly and downright embarrassing for a forward-looking state like Connecticut to inhibit a technology that could make people better off at a lower cost.
*These figures are based on the May 2016 Occupational Employment Statistics from the BLS. See this page for a list of top-paying states for optometrists. This data does not cover self-employed workers.