When Congressional Democrats began the legislative process to enact President Biden’s Build Back Better agenda last month, Sen. Bernie Sanders insisted on adding a costly expansion of Medicare benefits to the bill. But a new report from the program’s trustees makes clear that this expansion would be unwise: Medicare is already expensive and growing faster than the revenues needed to finance it, resulting in unsustainable deficits. Before Washington considers adding benefits that would further increase costs, it must find a way to pay for the promises it’s already made. Otherwise, critical public investments in young Americans and working families in greater need could be crowded out.
Debate among Democrats on the size and scope of their Democrat-only reconciliation package threatens to derail their biggest opportunity to make progress on long-held health care priorities.
But not only is the Democrat-only social spending bill in jeopardy, but disagreements over topline spending also threatens to derail the bipartisan infrastructure package. Progressives in the House want to wait to vote on the bipartisan infrastructure deal until the Senate has approved the Democrat-only reconciliation package, but nine moderate Democrats are pushing Speaker Pelosi to pass the infrastructure bill now as finding consensus on the social spending provisions could take months.
As House Democrats continue to battle it out, the Senate is moving forward with drafting the reconciliation package. It approved a topline $3.5 trillion budget resolution last week. The resolution directs the relevant committees to draft legislation to be included in the budget reconciliation package that will only require a simple majority, and Democratic votes, to pass. But requiring only Democratic votes still requires stitching together a constituency that includes both Congresswoman Alexandria Ocasio Cortez, D-N.Y., in the House and Senator Joe Manchin, D-N.Y – which currently seems elusive.
The health care provisions taken together are estimated to cost more than a third of the $3.5 total spending. They include:
Adding dental, vision, and hearing coverage to Medicare
Making the expanded Affordable Care Act (ACA) subsidies permanent
Closing the Medicaid gap in non-expansion states
Expanding home health services for seniors in Medicaid
Lowering the age of Medicare eligibility
Funding pandemic preparedness
Allowing the government to negotiate prescription drug prices
With health care, getting Democrats on the same page is never easy. Arizona Senator Kyrsten Sinema has already voiced her opposition to a package of that magnitude. So as the Democrats continue to debate what should be included, it is important that they consider the costs, impacts and potential pay-fors.
Adding dental, vision, and hearing coverage to Medicare
Senator Bernie Sanders, I-Vt., and progressive Democrats are leading the push for the inclusion of dental, vision and hearing coverage to be covered under the traditional Medicare program. While Medicare Advantage often covers dental, vision and hearing care, the traditional fee-for-service program, in which two-thirds of beneficiaries are enrolled, doesn’t. Adding dental, vision and hearing benefits to Medicare Part B would benefit millions of American seniors that currently can’t afford dental, vision and hearing services. While beneficiaries pay premiums for Part B, it’s largely subsidized by taxpayers. Which means the largest expansion of the Medicare program since the creation of Part D would come with a hefty price tag: roughly $358 billion over 10 years — but once fully phased in, it would cost roughly $80 billion per year. However, this provision that the Democrats are considering would impact the largest number of Americans — somewhere around 40 million seniors would be newly eligible for these benefits. Liberal Democrats have been outspoke proponents of expanding Medicare to cover dental, hearing and vision and a bill in the House that would do so has 76 co-sponsors.
Making the expanded ACA subsidies permanent
Democrats are also pushing to make the expanded subsidies for ACA plans approved in the COVID-19 relief law permanent. The American Rescue Plan expanded health insurance exchange subsidies to cover those making more than 400% of the federal poverty level (FPL) and increased the amount of subsidy for those making between 100-400% of the FPL. These enhanced subsidies make private coverage more affordable for the roughly 14 million people who buy coverage through the exchanges. However, it too, comes at a cost. It would cost roughly $165 billion over 10 years. And while these subsidies make coverage more affordable, they also flow to private insurance companies and hospitals with no mechanisms in place to reduce health care costs — which is the highest of all comparable countries. This has broad support across the Democratic coalition — including the more conservative Blue Dogs.
Closing the Medicaid gap in non-expansion state
In red states that have not expanded Medicaid, roughly 2.5 million people have incomes that are too low to qualify for subsidies for ACA plans, but do not meet the qualifications for Medicaid under the traditional program (being disabled, pregnant, or a child). Closing the so-called “Medicaid gap” is a priority for the Biden administration. Democrats are seeking a way to get these people coverage even if their states don’t expand the Medicaid program. The budget reconciliation package proposed creating a new federal program that would cover those in the Medicaid gap if their state hadn’t expanded the program. Depending on how it is structured, it could cost $300 billion over 10 years. Democrats in the New Democrat Coalition have said that closing the gap is a top priority but haven’t explicitly endorsed creating a new program to do so.
Expanding home health services for seniors in Medicaid
President Biden has proposed a $400 billion Medicaid funding increase for long-term care benefits as part of his American Jobs Act. The proposal would increase funding for long-term care and make it easier for states to use Medicaid resources on in-home care rather than at a facility. President Biden is trying to thread the needle between signaling that long-term care needs a dramatic increase in investment and not fleshing out the details to generate opposition. This was not included in the bipartisan infrastructure deal and now is being considered for the final reconciliation package.
Lowering the age of Medicare eligibility
Progressive Democrats see the reconciliation package as an opportunity to act on long-held goals, like expanding Medicare. They want to use the all-Democrat deal to lower the age of eligibility. However, it seems unlikely that the more conservative Democrats in the House and the Senate would support this effort and, to-date, there isn’t a formal cost estimate from the Congressional Budget Office (CBO). Roughly 8% of people 60-64, 1.6 million people, are uninsured and would benefit from an expanded Medicare program. However, if the program is expanded as is, it could also be cost effective for many people with commercial insurance to enroll in Medicare instead. This would make the expansion extraordinarily expensive. A more cost-effective way to expand coverage would be to allow people to buy into Medicare, covering the cost of their premiums. There could be a premium subsidy similar to that of the ACA but not as fully subsidized as the traditional program. This could help more people get access to the benefits of the program (lower prices, comprehensive coverage) without draining federal coffers.
Lowering the eligibility age faces an uphill battle. Not only is it extraordinarily expensive, but it is also is vehemently opposed by hospitals who prefer higher paying private insurance to Medicare rates. Senator Bernie Sanders, I-V.T., has long pushed to expand Medicare. However, he doesn’t have the support of all the other 49 Democrats that would be required to approve it. He is likely including this in the initial draft as a negotiating tool to press for other priorities (like a dental benefits expansion).
Funding pandemic preparedness
President Biden proposed $30 billion for future pandemic preparedness in his American Jobs Plan. President Biden had pushed for proactive investment to restock the Strategic National Stockpile, invest in vaccine development, and finance in U.S. production of personal protective equipment. But in an effort to squeeze a multitude of Democratic policy priorities into the $3.5 trillion reconciliation package, some are pushing to reduce pandemic preparedness funding to $5 billion. This seems shortsighted after the U.S. was unprepared for COVID-19 and ravaged by the novel virus.
Allowing the government to negotiate prescription drug prices
The only health care provision Democrats are considering that would lower health care spending is authorizing Medicare to negotiate drug prices for beneficiaries and private plans. One proposal being considered, H.R. 3, requires the Secretary of the Department of Health and Human Services (HHS) to negotiate the price of at least 50 brand-name drugs without generic competitors starting in 2025 and would make the negotiated price available to both Medicare and private payers. The CBO projects that Medicare drug negotiation would save $400 billion. However, the leverage to negotiate with drug manufactures comes from the government’s ability to refuse to cover a drug if it is too expensive. This may limit or delay the availability of some drugs for seniors in the Medicare program. It is likely that pressure from beneficiaries or specific advocacy groups may limit the government’s ability to refuse to cover certain high-cost drugs. If this is the case, the savings will likely be less than $400 billion. While this is the pay-for for many of the Democratic priorities, at this point it’s unclear if Democrats will come to an agreement on the best policy to reduce the cost of prescription drugs. Senator Ron Wyden, chairman of the Senate Finance Committee, and President Biden have also endorsed Medicare drug negotiation which suggests that it’s a priority to find a path forward to reduce the costs of prescription drugs but other Democrats are concerned that limit drug prices would also limit drug research and development.
As Democrats are working to reach a consensus on which health care provisions to include in their reconciliation package, they should consider how to reduce the topline number while achieving as many of their policy goals as possible. The savings from Medicare drug negotiation may not be as high as projected, depending on how the program is structured, so it is vital to include other ways of reducing health care costs. Program expansions should be accompanied with cost saving measures to reduce overall health care spending and make affordable health care coverage a reality for every American.
This week, the Innovation Frontier Project, a project of the Progressive Policy Institute (PPI), released a new report from Claudia Persico, an economist and leading environmental and health policy expert, on how exposure to pollution and lead negatively impacts the American workforce and economy.
“Lead and other environmental pollutants are not only causing a public health crisis, but they are hurting the productive capacity of the American people. Children who might otherwise have grown up to invent a new supercomputer or to cure a disease are having their brain function impaired at an early age by these pollutants,” said Caleb Watney, Director of Innovation Policy at PPI.
As outlined in this must-read new report, exposure to pollutants can cause cognitive impairments, behavioral issues, and lower test scores among children. Over a lifetime, these deficits in human capital accrue through lower educational attainment, wages, and productivity. The prevalence of pollution exposure is a significant obstacle to improving health, education, and economic growth in the United States.
Persico argues Congress, the White House, and state governments should use a variety of strategies to target pollution remediation for communities that disproportionately live and attend school near pollution sites, or live near high-risk sites, or live in older homes with pipes and paint that release lead into the air and drinking water. Persico suggests regulators act quickly to:
Raise Clean Air Act standards to close racial gaps in pollution exposure
Change zoning laws to keep children, schools, and daycares away from toxic sites
Accelerate cleanup of Superfund, Toxic Release Inventory, and other toxic sites.
Remediate homes with flaking lead paint to reduce blood lead levels in children
Increase lead screenings for children and use results to target homes for remediation
Use infrastructure spending to replace HVAC systems in schools and lead pipes in homes
Based in Washington, D.C. and housed in the Progressive Policy Institute, the Innovation Frontier Project explores the role of public policy in science, technology and innovation. The project is managed by Jack Karsten. Learn more by visiting innovationfrontier.org.
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
The Affordable Care Act (ACA) instituted new regulations on health insurance plans. One of the biggest changes was that large health plans are now required to spend 85% of health insurance premiums on health care services and smaller and individual health plans are required to spend 80%. The remaining 15% – 20% of premium revenues can be used for administrative costs and profits. These so-called Medical Loss Ratio (MLR) rules require that plans return excess premium revenues as rebates to beneficiaries.
In a year like we just had, where consumption changed dramatically from what health insurance actuaries predicted, MLR rebates protect consumers. Health insurers are returning $2.1 billion in MLR rebates in 2021 because people used fewer health care services in 2020 than had been anticipated and priced into premiums.1
But dental insurance plans were exempt from ACA reforms and are not subject to these MLR rules. Some dental health plans have spent as little as 4% of premiums on actual dental care.2 Additionally, they typically have annual maximum benefit limitations and high cost-sharing. All and all, patients often get a bad deal on dental health plans.
Last year, spending on dental services dropped 20%.3 But most consumers and employers won’t see that money returned to them through rebates. Instead, it will line the pockets of dental insurance companies as a nice windfall.
But if we wouldn’t let health plans keep the excess premiums, why do we continue to let dental health plans go unchecked? This brief
outlines why it’s important to subject dental health plans to the same regulations as medical health insurance.
BACKGROUND
It’s an accident of history that oral health is treated separately from our medical system. When early dentists wanted to join the Medical College at the University of Maryland, the physicians refused them entry. Dentists set up their own line of study and that divide lives on. Fewer than 1% of health plans include dental benefits — usually dental health plans are purchased separately, often from a different company — to fill in what health plans leave out.4
Roughly 80% of Americans have some form of dental coverage.5 Of those with coverage, roughly two-thirds have private dental coverage, usually offered by an employer, though about 7% of Americans buy stand-alone dental plans through or outside of the ACA exchanges.6 Of those with private coverage, 77 million are in self-insured plans that are governed by the federal government and 88 million are in plans that are regulated by the states7. The remaining third have publicly funded coverage through Medicaid, CHIP, TriCare, or Medicare Advantage.
But even those who have employer-sponsored dental coverage often don’t get a great deal. A typical dental insurance plan offers what is known as”100-80-50″ coverage. This means the plan will pay 100% of the cost of routine preventive cleanings. Then it will cover 80% of the cost of basic services such as fillings or root canals, and 50% of the cost of major procedures such as crowns and bridges. Usually, there is a maximum benefit of $1,000-$2,000 per year. While only 6% of people exceed their maximum benefit per year, requiring one crown can cost over $2,000 — blowing through the maximum benefit.8
Dental costs have been increasing for decades. Between 1996 and 2016, per capita dental care expenditures increased 27%.9 Expenditures for dental services increased from $43 billion in 1996 to $96 billion in 2015 — a 200% increase.10 In 1996, the mean annual expense for a dental visit was $374, or $564 when adjusted for inflation, but by 2015, that had increased to $696. But the average dental plan benefit has not changed in 50 years. In 1970, a $1,000 benefit was worth about $6,909 in 2021 dollars.11 Yet, some plans still have a $1,000 maximum benefit in 2021 which no longer provides the same level of coverage because of inflation.
America is at a COVID-19 crossroads.For the first time since the highly effective vaccines became widely available in the spring,the new case rate is back on the rise due to the spread of the more contagious delta variantand the stalled effort to vaccinate people in many parts of the country.
According to medical experts, reaching herd immunity will require that 70% to 90% of the U.S. population be fully vaccinated. But despite having enough vaccines available to inoculate every eligible American age 12 and up, just under 50% of the U.S. population is fully vaccinated.
Worse, at the current vaccination rate of roughly 500,000 per day, it will take nine more months to cover just 75% of the population. This would give dangerous and more contagious COVID variants a chance to gain a foothold and perpetuate the pandemic.
Contain COVID at transportation hubs
President Joe Biden and COVID czar Jeff Zients deserve tremendous creditfor making the COVID-19 vaccines widely availableand bringing focus and discipline to the White House pandemic dysfunction they inherited from former President Donald Trump. But a reliance on incentives and awareness can only get us so far, especially when some irresponsible politicians have been stoking vaccine skepticism and outright hostility.
To get to herd immunity within a reasonable time frame, the Biden administration is going to need to add to its arsenal some targeted vaccine mandates— and the obvious first step is to require proof of vaccination when embarking on an airplane.
According to a number of legal experts, the president has the authority – from laws establishing the Centers for Disease Control and Prevention and the Federal Aviation Administration, as well as the Commerce Clause of the Constitution – to require all airlines to ask ticket holders to provide proof of full vaccination.
By disrupting the spread of COVID-19 at transportation hubs where individuals gather and connect to other geographic regions, and by creating another incentive for adult vaccination, an airline vaccine requirement would help bring the pandemic to an end.
No doubt even a targeted mandate for airline passengers will stoke the outrage machine at Fox News and other right-wing propaganda outlets. Republicans eager for Trump’s favor and anti-vaxxers can be expected to decry any vaccine requirement as an attack on Americans’ basic “freedoms.”
Nowhere in the Constitution’s Bill of Rights will conservatives find a right to infect others with a deadly disease. In addition to defending our civil liberties, government is responsible for promoting the general welfare and protecting citizens from harm. No rational person considers requiring a license to drive a car or fly a plane a form of tyranny.
Citizens have responsibilities, too – to each other, their communities and their country. In times of war and other national emergencies, Americans have always proved willing to sacrifice their private interests and pursuits for the common good. Amid a resurgence of COVID-19 and pervasive vaccine hesitancy, we face just such an emergency today.
Treading cautiously isn’t working
That’s why it is deeply unpatriotic for anti-vaxxers to feed the public misinformation about the efficacy and safety of vaccines. It’s also reckless. More than 99% of people dying from COVID-19 are unvaccinated, according to Surgeon General Vivek Murthy.
President Biden would be on solid ground in invoking the principle of mutual responsibility as a counter to the right’s strangely anti-social conception of freedom. A vaccine requirement for air passengers wouldn’t force anyone to get vaccinated; it would leave them to choose whether refusing the vaccine is more important to them than being able to fly.
In purely legal terms, the Biden administration is well within its authority to protect the health and safety of passengers and citizens. Politically, the president and the COVID-19 vaccines are already under attack by extremists, and this will only get worse should cases rise again and we see the return of mask mandates, such as the one just reinstated in Los Angeles County.
The debate over vaccinations is polarized, and the Biden administration has been right to tread cautiously. But if the best we can do under our current strategy is less than what we need for herd immunity, then reasonable, targeted mandates will be needed in order to end the pandemic and ensure the health and safety of all Americans.
Paul Weinstein Jr. is a senior fellow at the Progressive Policy Institute and directs the M.A. program in public management at Johns Hopkins University. Will Marshall (@Will_PPI) is the president of the Progressive Policy Institute.
A new paper released today by the Progressive Policy Institute examines two key questions facing the biotech industry in America and the European Union (EU): Is it pro-innovation for European antitrust regulators to have the power to block a deal involving two American biotech companies that do no substantial business in Europe? And, under what conditions is vertical integration a socially beneficial strategy for accelerating innovation?
The paper, titled “Biotech Innovation: Two Important Questions,” is authored by Dr. Michael Mandel and Alec Stapp.
“There is little evidence that most vertical acquisitions are anti-competitive. If our shared goal is to support innovation and scaled production of potentially-lifesaving drugs and medical products, the U.S. and E.U. governments should work to advance integrated development — not regulatory imperialism,” said report authors Dr. Michael Mandel and Alec Stapp.
The paper examines the proposed purchase of cancer-diagnostic developer Grail by gene-sequencing leader Illumina. The Federal Trade Commission (FTC) recently intervened to stop the acquisition, worried that Illumina would block potential competitors of Grail from using its gene sequencers. The FTC ultimately dropped its case, instead allowing the European Commission to take the first swing at blocking the acquisition. The EU will rule by late July on the merger.
The paper concludes that excessive antitrust focus on blocking vertical integration in the biosciences could impede the development of important new products and treatments (though so-called “killer acquisitions” are an important exception that warrant increased scrutiny from regulators). The paper also broadens the scope of the issue, extending beyond the Grail and Illumina case and into the larger climate of regulation, innovation, and integration in the EU and U.S.
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
Editor’s note: Throughout this piece, “prison” is used to represent places of detention, including county and regional jails, federal and state prisons, and juvenile detention facilities. Data from The New York Times includes immigration detention centers as well.
Women Behind Bars: Violence and Neglect During the Pandemic
Despite accounting for only four percent of the world’s female population, the United States houses more than 30 percent of the world’s incarcerated women. This rate has increased nearly 800 percent since the 1970’s. These inmates face a harsh and restrictive prison environment designed for violence-prone men, and the emergence of the pandemic has only further opened the doors for inhumane treatment. Prisons are among the primary hotspots for the coronavirus, with infection rates three times that of the general public. As the virus surges through correctional facilities, inmates are not able to social distance, quarantine, or benefit from adequate medical treatment. Depleted resources and insufficient space, combined with a vulnerable population, created the perfect storm for Covid-19 to spread quickly.
Inside the Danbury Federal Correction Institution in Connecticut, dozens of women tested positive with no space to quarantine. To prevent the virus from spreading, they were housed in the inmates’ waiting room with no beds, only rudimentary restrooms, and no place to bathe (although showers were eventually installed.) During months when nighttime temperatures still dipped below freezing, the women were instructed to assemble and to sleep on metal beds, with limited mattress availability. They lacked substantial food and were generally not granted over-the-counter medication except Tylenol. One sick inmate was hospitalized for dehydration, and many were left in the locked visiting room without attention to their severe symptoms. Despite these worsening conditions during the pandemic, the Connecticut Department of Correction claimed that Covid positive inmates were “provided medical care in accordance with CDC guidelines.” Stacy Spagnardi, an inmate at Danbury currently in home confinement, recalls something very different: “We were all thinking we would die in there, and nobody would know until count.”
If there is any silver lining to the misery inflicted by the pandemic, it is that the virus turned a spotlight on the lack of adequate healthcare in our country’s prisons, especially for women.
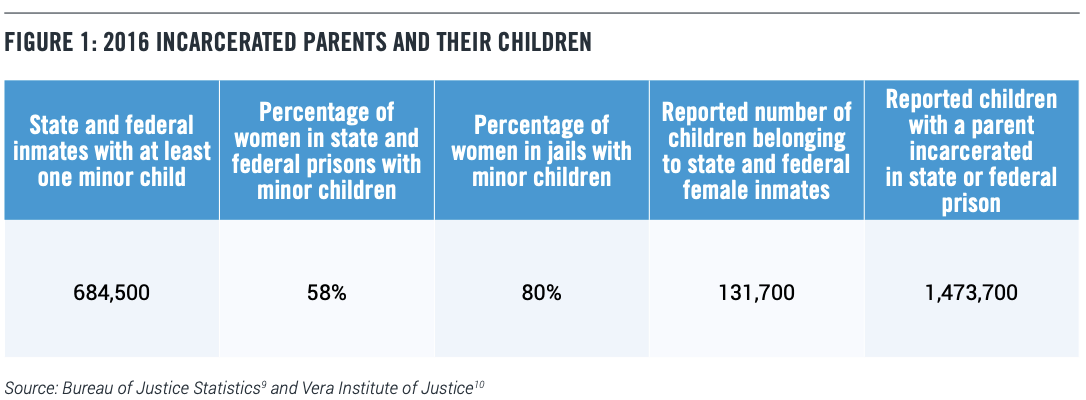
This is particularly true, for example, in the case of prenatal care. Roughly four percent of all newly incarcerated women arrive to serve their sentences while carrying a baby. On average, 2,000 children are born behind prison walls every year. While in prison, only 58 percent of pregnant women report receiving any prenatal care. The Prison Policy Institute found that 31 states lack any nutritional plan or dietary supplements for incarcerated pregnant women, a key component to delivering a healthy child. As a result, many expecting mothers in jail suffer from malnutrition.
Female inmates, many of whom were physically abused or addicted to drugs before their arrests, need better health care. This is especially true for women experiencing high-risk pregnancies because of their struggles with substance abuse.
Women in jail often give birth alone in their cells with no medical aid or assistance. Prisons also have been known to shackle or otherwise restrain inmates during labor. This increases risk by limiting the women’s movement, increasing pain, and obstructing the diagnosis of complications during birth.
After an often-precarious delivery process, most women are separated from their children within 24 hours. Their babies are placed with a relative, adoption family, or into foster care. Maternal separation, of course, can be highly traumatic to both mother and child. For the mother, it’s an additional harsh punishment over and above their sentence. For the newborn, separation can cause emotional and behavioral problems that can last a lifetime.
Research suggests that children born to imprisoned parents experience psychological and educational problems, such as higher rates of depression and suicide, antisocial behavior, learning disabilities, and behavioral issues that result in suspension or expulsion from school. On average, children with incarcerated parents are six times more likely to become incarcerated themselves.
Covid-19 has made prison even more perilous for pregnant women. Consider the case of Andrea Circle Bear, who was pregnant and serving a two-year sentence for selling drugs on the Cheyenne River Indian Reservation. Circle Bear contracted Covid-19 in the overcrowded prison in Fort Worth, Texas. She was on a ventilator when the time came to give birth. Three weeks later, she was the first federal female prisoner to die from Covid-19. “Not every prison death is avoidable, but Andrea Circle Bear’s certainly seems to have been — she simply should not have been in a federal prison under these circumstances,” contends Kevin Ring of Families Against Mandatory Minimums.
For Circle-Bear and other non-violent offenders, early release or home-confinement policies could have prevented unnecessary sickness and death behind bars, but many states made few efforts to reduce their prison populations amidst the pandemic. In states that did try to halt Covid-19’s spread in their prisons, the response was uneven. Some states enacted limited early-release programs. A handful of governors have issued executive orders to grant early release for certain inmates, while the Federal Bureau of Prisons transferred some into home-confinement.
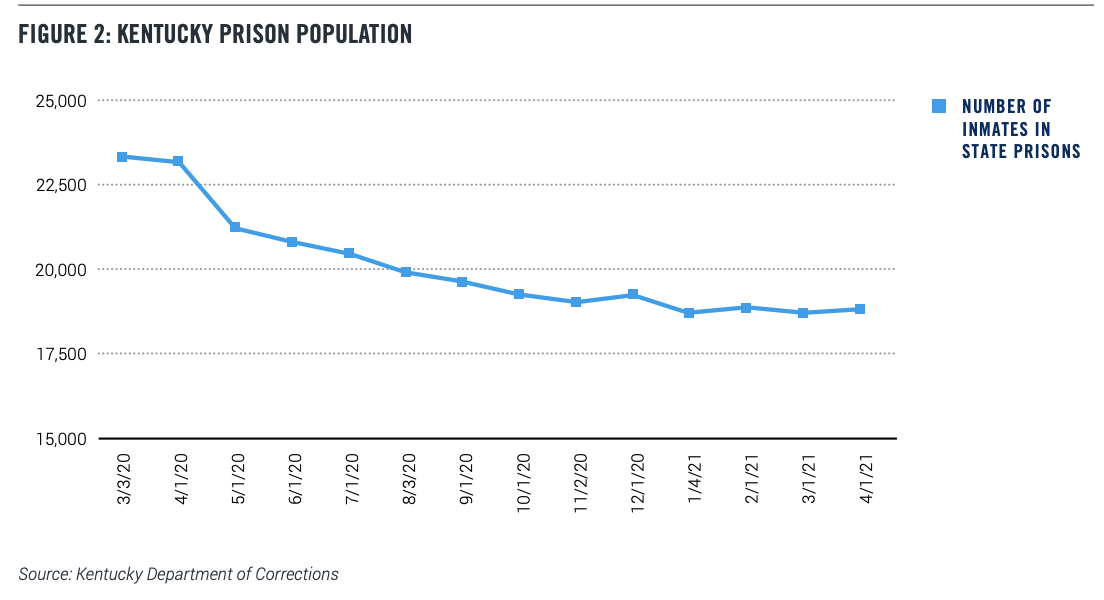
For example, Kentucky’s public defenders, prosecutors, Supreme Court, county jails, and Gov. Andy Beshear worked together to reduce Kentucky’s prison population. Those who were medically vulnerable, low-risk, or near the end of their sentences received priority in early release policies.
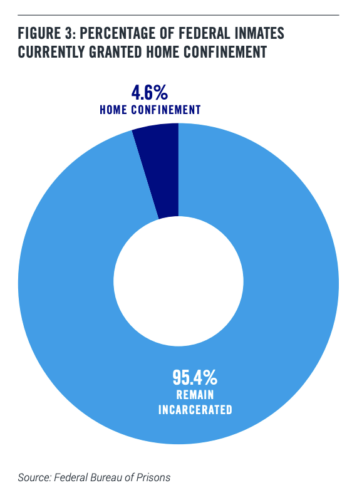
Of the 152,124 prisoners currently under federal jurisdiction, 7,314 have been placed in home confinement. The Attorney General released a memo in March of 2020 instructing the Federal Bureau of Prisons to allow inmates to serve out their sentences at home when appropriate. Since then, 24,668 inmates have been granted home confinement.
In April of 2020, Pennsylvania’s Governor Tom Wolf began the Temporary Program to Reprieve Sentences of Incarceration. Although the plan originally estimated that 1,800 inmates would qualify for reprieve, only 159 individuals were released through this program.
In an effort to reduce Covid-19 transmission, some states also have restricted the number of security guards on staff. Unfortunately, this has had the unintended consequence of making women more vulnerable to sexual assault and abuse. According to the U.S. Bureau of Justice Statistics, 42 percent of sexual abuse in prisons is perpetrated by staff, while 58 percent is perpetrated by other inmates. However, this data reflects only substantiated sexual assault claims, which amounted to 5,187 of the 67,169 allegations from 2012-2015, or just eight percent of all claims. While it would seem that having less prison guards would reduce the number of potential abusers, a lack of security can empower predatory staff or inmates to commit sexual assault without supervision.
Sexual abuse is a notorious aspect of prison life for men and women. But it’s a special problem for women, a majority of whom previously have been victims of physical and/or sexual assault. The cycle of abuse continues in prison. The Department of Justice found widespread rape and sexual harassment inside the Julia Tutwiler Prison for Women in Alabama and the Edna Mahan Correction Facility for Women in New Jersey. Along with suffering severe mental and physical trauma, several women became pregnant after being raped by guards. The DOJ argued that these conditions violated women’s eighth amendment rights against “cruel and unusual punishment.” But under Covid protocols that limit personnel and surveillance, more women are at risk in understaffed facilities like Edna Mahan and Tutwiler.
Covid-19 also has created new stresses on female inmates’ social and emotionalwell-being. In addition to the life-threatening physical conditions during the pandemic, incarcerated women also are subject to the misuse of punitive policies like solitary confinement and terminated phone and visitor access that can impair their mental health. The use of solitary confinement as a blunt instrument for enforcing social distancing during the pandemic has increased 500 percent. Yet solitary confinement is known to increase anxiety and suicidal thoughts, particularly in women who have suffered sexual abuse and feelings of low self-worth. Prisons need to be more careful in calculating the trade-off between protecting inmates from Covid and endangering their mental health.
Covid-related policies preventing communication between incarcerated mothers and their children also have strained family relationships. As the general population has relied on technology to stay in touch with our loved ones, many prisons have restricted access to the phone and eliminated visitation. An overwhelming majority of female inmates are mothers, and these policies can degrade their mental health by cutting off communication with their children.
What Should be Done?
Even as Covid cases plateau nationwide, Covid-19 infections continue to rise in jails and prisons. Moreover, new variants found in Michigan, Colorado, and other states pose fresh dangers of contagion, since prison staff can carry the virus in and out of prison from these hotspots.
The task of mitigating the pandemic inside our jails and prisons is complicated by the fact that a multiplicity of federal and state jurisdictions cut across the U.S. criminal justice system. States decide their own policies, whether for early release programs, vaccine rollout, or correctional institution budgeting. As a result, prisoners across the country experience a variety of conditions and Covid-19 protocols.
“If there was clearly a right strategy, we all would have done it,” said Dr. Owen Murray, a physician in charge of correctional healthcare at dozens of Texas prisons. Nonetheless, America’s correctional facilities have a myriad of ways to create more humane and safe conditions for inmates:
Increase testing and dedicate spaces for quarantine. The first step is better measurement of the challenge. Correctional facilities should test all staff and inmates routinely and release results publicly. To limit transmission of the virus, symptomatic inmates should be placed in a separate space from other prisoners while they wait for their results. These areas should be adequately climate controlled and fully equipped with food, water, sanitary and medical resources, books or other sources of entertainment, and working phones for communication with loved ones during this short isolation period.
Prioritize inmates in vaccine distribution. The CDC and the American Medical Association have recommended that vulnerable populations, including incarcerated individuals, be given priority for receiving vaccines. Overcrowding, lack of medical care, and an at-risk population has made Covid-19 an even deadlier threat inside prisons. The federal prison system has administered at least the first vaccine dose to about 146,972 of its approximately 152,124 federal prisoners. However, vaccine distribution inside state correctional facilities is controlled by the state government and varies widely across the country. In Florida, no inmates in state correctional institutions have received the vaccine. Contrastingly, Kansas has vaccinated about two-thirds of its 8,700 inmates. Kansas Governor Laura Kelly faced intense political resistance to prioritizing inmates in vaccine efforts, but as John Carney, a member of the Kansas Coronavirus Vaccine Advisory Council explains, “All of us kind of came around to this notion that the most vulnerable is the most vulnerable.” Inmates should be considered high priority in state and federal vaccination efforts, especially now that the national vaccine supply has increased and shots are more readily available.
Adopt alternate forms of sentencing. When possible, courts and lawmakers should seek alternatives to incarceration, especially for non-violent offenders, to decrease the number of people in prisons nationwide. Fewer people entering correctional facilities means more room for social distancing, resources for other prisoners, and fewer Covid cases. Drug courts, fines, restitution, community service, probation, house arrest, psychiatric treatment, and work release are other plausible avenues to explore.
Increase and improve medical care for inmates. Correctional facilities should be given the resources to hire more medical staff trained to recognize inmates‘ Covid-19 symptoms and treat them appropriately, move prisoners to the hospital if their conditions become serious or require more equipment than on hand, and frequently monitor inmates’ health.
End solitary confinement for at-risk prisoners and as a method for social distancing. State and federal jails and prisons should be prohibited from using solitary confinement as a means of quarantining inmates. The practice can particularly harm pregnant women or those with underlying health conditions. New York recently ended long-term solitary confinement and banned the practice entirely for minors and pregnant women; correctional facilities should follow this lead to protect vulnerable inmates from the severe mental health ramifications caused by this isolation.
Reopen libraries and educational programs. In keeping with CDC guidelines, prisons should reinstate these crucial educational spaces and programs. Inmates who participate in educational programs have a lower rate of recidivism, higher rate of literacy, increased employment opportunities upon release, and receive fewer disciplinary infractions. The Utah State Prison houses five libraries with an array of books to keep inmates engaged and busy. Camille Randles, an inmate who regularly uses the women’s prison library, explains how books are a “safety net” that allow inmates an escape from reality. The prison also offers programs on substance abuse and sex-offender treatment that can help inmates gain parole upon graduation. The largest meta-analysis on correctional educational studies found that inmates participating in educational programs are 43 percent less likely to return to prison than those who do not. These programs are also cost-effective, reducing incarceration costs by $4-5 for every dollar invested in correctional education programs. If all safety precautions and social distancing measures are enforced, the benefits of these programs towards limiting future incarceration and reducing costs far outweigh the risk of transmission.
Allow for greater virtual communication. To connect prisoners with their families and attorneys, prisons should end restrictive communication policies and install video conferencing, increase access to phones, and expand computer usage. These shared tools and spaces should follow CDC guidelines and be thoroughly cleaned between prisoner use. They will allow incarcerated individuals to better communicate with their loved ones, which also has been shown to reduce recidivism by strengthening family support before the re-entry experience.
Institute job training programs. One of the largest obstacles for people re-entering society is securing a well-paying job. Job training programs equip inmates with the skills and confidence they need to be successful in the workforce and increase odds of employment by 28 percent. Some programs, like Trades Related Apprentice Coaching, partner with local businesses or labor unions to place women in jobs once their training is complete. Crystal Lansdale, an inmate at Washington Corrections Center for Women, explains, “The construction trades is something like a way out of the box for me. I need a career that is going to give me retirement, that’s going to give me benefits, that’s going to give me an opportunity to take care of my kids.” Many people like Crystal need legitimate work to support themselves and their families once they are out of prison. Furthermore, certain programs should be tailored specifically to youth workforce development, so that juvenile offenders can form connections with professionals and mentors that can influence them during their developmental years as well assist them in entering the workforce. The DOJ’s National Institute of Corrections highlights how building “employable skills” for incarcerated youth increases safety in the community and advances employment opportunities for juvenile offenders.
Improving Conditions for Women
In addition to these general reforms, policymakers should adopt specific strategies for creating more safe and humane conditions for incarcerated women vulnerable to ill-health, neglect and abuse:
Report accurate, disaggregated data. Providing disaggregated data will help to gauge the pandemic’s effect on incarcerated women and minorities. Only then can policies be designed to better encompass their needs. Congress should pass the Covid-19 in Corrections Data Transparency Act introduced by Representative Clarke, Garcia, and Pressley alongside Senators Warren, Murray, Booker, and Kelly. The legislation would require the Federal Bureau of Prisons, the U.S. Marshall Service, and state and local governments to report disaggregated Covid data for federal, state, and local correctional facilities.
Prioritize women in early release policies. According to The New York Times, only about 5 percent of prisoners currently serving federal sentences have been granted home confinement. Some governors have implemented early release policies, but not at the rate that various prosecutors, judges, and interest groups have called for. Pregnant women, women in prison for non-violent offenses, and women with pre-existing conditions should be prioritized for early release. A two-year stint for selling drugs should not be a death sentence. Women also have a lower rate of recidivism than males, indicating that early release plans would not encourage future crime.
Increase and improve prenatal care. Comprehensive prenatal care should be extended to all pregnant inmates to decrease the risk of serious complications if they contract Covid-19. The House in October 2020 passed the Protecting the Health and Wellbeing of Babies and Pregnant Women in Custody Act, which dictates that the Bureau of Justice reports annual data on the demographics and health needs of pregnant women in custody, prohibits the use of restraints on pregnant inmates, and provides appropriate services, health care, and nutrition for pregnant women. The Senate should act quickly to pass this bipartisan bill.
Train, recruit, and oversee more qualified guards and officials. Improving the quality of prison staff is a key step toward increasing safety for female prisoners. Monitoring guards on duty, hiring more female officers, and educating personnel around the specific challenges incarcerated women face can decrease sexual assault and violence in prisons.
Provide enhanced nutritional options for female prisoners, especially pregnant women. According to national guidelines, women generally need more nutrients than men, especially for a healthy pregnancy. A balanced diet including folic acid, iron, calcium, zinc, and Vitamin D will help strengthen prisoners’ immune systems to fend off the virus and deliver healthier babies.
Supply adequate cleaning supplies and feminine hygiene products. Many states are not required to provide incarcerated women with menstrual products. In Alabama’s Tutwiler Prison for Women, the Department of Justice found that male guards withheld menstrual items unless prisoners would have sex with them. Correctional facilities should provide feminine hygiene products to all incarcerated women to ensure their basic needs are met. In addition, correctional facilities should be equipped with various cleaning supplies to limit transmission of the virus.
Conclusion
Prisons are dangerous places for everyone, especially women. The pandemic introduced a new threat to incarcerated women’s existing conditions of violence, sexual assault, and neglect. To make prisons safer for women, legislation must address the structural issues plaguing the criminal justice system. As the country works to rebuild itself, women in prison continue to struggle against mass incarceration, gender discrimination, and punitive methods. The pandemic magnified many of these issues and crafting a gendered response to the virus is the first step toward treating incarcerated individuals with respect and human dignity.
In his first joint address to Congress, President Biden made it clear that he plans to go big on many health care issues including expanding the Affordable Care Act (ACA), reforming drug pricing, and even “ending cancer as we know it.” But he was scant on details and Democrats in Congress are nervous that if he doesn’t act soon, the window for health reform will close with the 2022 midterms.
Everyone agrees that passing health care reforms won’t be easy with paper-thin Democratic majorities in the House and Senate – especially when Democrats themselves disagree over the course Biden should take.
Last week, the pragmatic New Democrat Coalition urged the president to include in his American Families Plan several policies that would “strengthen and expand on the ACA:”
Making the American Rescue Plan’s increase and expansion of ACA subsidies permanent
Giving holdout states 100 percent federal match if they expand Medicaid (meaning the federal government would cover the entirety of the cost)
Automatically enrolling those eligible for Medicaid and fully subsidized ACA plans
Meanwhile, a group of left-leaning and moderate Democrats led by Reps. Pramila Jayapal and Conor Lamb – are encouraging the president to:
Allow Medicare to negotiate drug prices
Lower the age for Medicare eligibility
Expand Medicare coverage of dental, hearing and vision benefits
Senator Sanders and 17 other Senators also signed a letter encouraging President Biden to push for these expansions saying that, “the time is long overdue for us to expand and improve this program so that millions of older Americans can receive the health care they need, including eyeglasses, hearing aids and dental care.”
Rep. Frank Pallone and Speaker Nancy Pelosi have re-introduced the late Rep. Elijah Cummings’s bill HR 3, which seeks to cap Medicare beneficiary out of pocket drug spending and overhaul how Medicare pays for drugs.
Democrats aren’t just debating the contents of the President’s health proposals, they also disagree about legislative tactics: Some want the president to include his larger health care priorities in the next reconciliation package, which requires only a simple majority to pass. Others worry that if only one Democratic Senator breaks ranks, that tactic will fail and leave them empty-handed.
One thing is clear: Other than on drug pricing, Democrats are not pushing for policies that would rein in health care costs. Adding benefits is easy; controlling costs is hard.
The health care industry will always push back against measures that seek to limit health care spending.
But there is widespread support among corporate leaders and voters for more government action on health care costs. A new survey from the Kaiser Family Foundation and Purchaser Business Group found that corporate leaders think that the cost of health insurance will reach a breaking point in the next decade. To mitigate high health care spending, 83 percent said that a greater government role health care would be “better for business.” Specifically, the survey found support for:
Lowering Medicare eligibility age
Creating a public insurance option
Capping hospital prices caps
Drug price negotiation
A broader federal role in health insurance coverage
There is also bipartisan support for Medicare drug negotiation: KFF found that 89 percent of survey respondents support allowing the federal government to negotiate with drug companies to get a lower price on medications.
But how does President Biden balance public demands with the political pressures of a divided Congress and strong health care industry lobby?
Given that the cost of health care is a top concern of the public and employers, President Biden should pursue pragmatic policies that would rein in spending which would allow his administration to pursue more ambitious coverage expansions.
Creating an early Medicare buy-in: A Kaiser Family Foundation analysis found that health spending for 60- to 64-year-olds would be lower under Medicare than under large employer plans. Allowing this group to buy into Medicare earlier at a premium that fully covers the cost of their coverage is a politically popular idea that would reduce health care expenditures for both employers and the federal government because of the employer sponsored health insurance tax exclusion.
Encouraging states to expand Medicaid: Medicaid expansion has been passed by voter referendum in even the most conservative states, such as Idaho. The Biden Administration should push hold out states and provide additional financial incentives for states to expand Medicaid. It is a cost-efficient way of providing health coverage to low-income people.
Expanding ACA subsidies only with other cost controls in health care spending: Expanding the ACA subsidies, while an important step in getting more people insurance coverage, is the most expensive way to do so. The per capita cost for subsidizing ACA plans is more expensive than the per capita costs of Medicare and Medicaid. Making the enhanced subsidies permanent would cost $200 billion, roughly one-fifth the cost of the entire 2010 Affordable Care Act.
The health care industry supports making permanent the ACA subsidy expansions included in the American Rescue Act. When more people have access to affordable health insurance, hospitals, doctors, and drug companies are more likely to get reimbursed for the services they provide. However, these subsides should only be made permanent with some tradeoffs to rein in costs – these could include Medicare drug negotiation, price caps or a public option to compete alongside private health plans, but the administration should not authorize $200 billion in new health care spending without finding ways to curb the health care cost growth curve.
In general, it seems that most Democrats are tempering their expectations and pursuing realistic policy goals that can make it through a starkly divided Congress. But given the uncertainty of when the Democrats will have the trifecta of the White House, Senate and House again, they should use this time to pursue health care policies that will both expand coverage and reduce costs, making a real difference in people’s lives.
On Friday, April 23rd, PPI Director of Social Policy Veronica Goodman spoke with Professor Maya Rossin-Slater, a paid leave expert at Stanford University about her latest paper, The Impact of Paid Family Leave on Employers: Evidence from New York, co-authored with Ann P. Bartel, Christopher J. Ruhm, Meredith Slopen, and Jane Waldfogel. Watch the full interview below.
On this week’s Radically Pragmatic Podcast, Crystal Swann, Senior Policy Fellow at the Progressive Policy Institute and Mosaic Economic Project lead and Hilary Abell, Mosaic Economic Project Cohort member and co-founder of Project Equity, sit down with Rep. Chrissy Houlahan (PA-06), a trained engineer, entrepreneur and veteran.
Congresswoman Houlahan serves on the House Armed Services Committee, the House Foreign Affairs Committee, and the House Small Business Committee. Additionally, she is the Chair and Founder of the Servicewomen and Women Veterans Congressional Caucus, is Co-Chair of the Women in STEM Caucus, and is a Whip in the New Democrat Coalition.
They discuss the role of women in the new post-COVID economy, removing barriers to childcare, supporting access to capital for women of color seeking to become entrepreneurs, expanding access to affordable health care and more.
“There’s a lot of different very good ideas on how to make healthcare more accessible, more affordable, and more portable for people. Those three things are issues one, two, and three in my community and many other communities. People – whether they are individuals who have health care, individuals who don’t have health care, entrepreneurs who are starting businesses or larger businesses who employ people – whatever one of those things you fit into, you all have issues with health care. So we need to be thinking about how to make our collective systems more efficient and more fair,” said Rep. Chrissy Houlahan on the podcast.
This podcast was in partnership with PPI’s Mosaic Economic Project. The Mosaic Economic Project is a network of diverse and highly credentialed women in fields of economics and technology. Mosaic programming focuses on upskilling, connecting, and advocating for cohort participants’ meaningful engagement in public policy debates, with a particular focus on engaging Congress and the media.
The Progressive Policy Institute(PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
On this week’s Radically Pragmatic Podcast, PPI President Will Marshall and Center for New Liberalism Policy Director Jeremiah Johnson sit down with Rep. Stacey Plaskett, Delegate to the United States House of Representatives from the United States Virgin Islands’ at-large congressional district. Congresswoman Plaskett serves on the House Ways and Means, Agriculture and Budget Committees, and is a leadership member of the New Democrat Coalition.
They discuss the New Democrat Coalition’s 100 Days Agenda, and the need for continued coronavirus relief and recovery measures – especially for regions like the Virgin Islands. Additionally, Congresswoman Plaskett outlines the critical nature of the American Jobs Plan, and the need to invest in long-term resiliency measures like job training, infrastructure development and clean energy.
On this week’s Radically Pragmatic Podcast, PPI President Will Marshall and Senior Policy Fellow Crystal Swann sit down with Rep. Marilyn Strickland (WA-10), a former Mayor of Tacoma, and Sly James, former Mayor of Kansas City.
They discuss a new “metro-federalism” – the role of local leaders in effectively deploying the public resources provided by Congress in the American Rescue Plan Act, and how mayors will support the Biden Administration’s COVID-19 relief and recovery goals – often as Republican-controlled state legislatures are hostile to the new Democratic administration.
The leaders also discussed the American Jobs Plan, the Biden Administration’s next phase of the Build Back Better agenda, which will invest billions in traditional and human infrastructure so we can get every American – including women – back to work and back on track.
“We think about infrastructure as very traditionally roads, bridges, mass transit, sewers, et cetera. Now it includes broadband, now it includes affordable housing, and now it also includes what I call the “continuum of care-giving” – the way we care for our youngest and the way we care for our eldest, because when we talk about infrastructure as job creation, that is very male-dominated for a few reasons. But when we talk about the care-giving infrastructure, now we’re talking about more participation by women, and this is important because COVID has just disproportionately affected women’s participation in the workplace and on top of that women of color’s participation in the workplace. So we’re going to have a truly equitable and inclusive sustainable economic recovery, we have to look at the care-giving infrastructure as part of our holistic approach to how we invest in infrastructure,” said Rep. Marilyn Strickland on the podcast.
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
PPI President Will Marshall and Senior Policy Fellow Crystal Swann sit down with Rep. Marilyn Strickland (WA-10), a former Mayor of Tacoma, and Sly James, former Mayor of Kansas City.
They discuss a new “metro-federalism” – the role of local leaders in effectively deploying the public resources provided by Congress in the American Rescue Plan Act, and how mayors will support the Biden Administration’s COVID-19 relief and recovery goals – often as Republican-controlled state legislatures are hostile to the new Democratic administration.
The leaders also discussed the American Jobs Plan, the Biden Administration’s next phase of the Build Back Better agenda, which will invest billions in traditional and human infrastructure so we can get every American – including women – back to work and back on track.
The White House is currently considering whether to support a push to suspend drug companies’ patent rights to their Covid-19 vaccines. This is a delicate issue that requires policymakers to balance the importance of incentivizing medical R&D in the future against the need for a rapid vaccine rollout around the world — especially in developing nations. We need more manufacturing firepower, and the US can best unleash it by coordinating a global technology transfer through the purchase of the intellectual property and the creation of incentives for producers to share their know-how with the rest of the world.
The legal proceedings around this issue were triggered in October 2020, when India and South Africa circulated a World Trade Organization Trade-Related Aspects on IP Rights (TRIPS) petition calling for the intellectual property protections on Covid-19 vaccines to be suspended for the remainder of the pandemic. The movement has quickly gained momentum since.
More than 100 countries have signed on to the motion, some out of narrow concern with the pace of vaccine distribution in their country and others as a protest vote against a global IP regime they believe favors rich countries. But because WTO motions like this require unanimous approval from all members, the currently opposed group, which includes the US, EU, and the UK (not coincidentally the nations where the vaccine developers are located), is able to block the motion. In the last week or two, a group of House Democrats, with the support of Bernie Sanders and Speaker Nancy Pelosi, have started lobbying the Biden administration to switch course and support the motion.
The case for suspension:
The pro-suspension side is relatively straightforward. While wealthy countries have been able to receive quick access to the vaccine (indeed, near-miraculous progress compared to the normal vaccine creation timeline), deployment has been sluggish around the rest of the world and especially in developing nations. This is both a moral and a public health issue. It’s bad for people to die simply because they live in a country with fewer scientific resources. And the longer the virus hangs around, the higher the risk of a significant mutation that could restart the whole pandemic.
It’s difficult to project vaccine production timelines exactly, but a commonestimate from experts seems to be that many low-income countries won’t be fully vaccinated before the end of 2022. Others are more pessimistic, predicting immunity as late as 2024. Either way, that’s still quite a while away, and plenty of time for new Covid variants to emerge. Already we’ve seen the B.1.351 variant from South Africa poke holes in our defenses as it appears the AstraZeneca vaccine is significantly less effective against this strain. The Pfizer and Moderna vaccines still appear to offer good protection, but even they may see a small drop in effectiveness.
We can always create new vaccines or new booster shots to help address new variants, but the distribution map is going to be similarly skewed towards rich countries. A cycle in which rich countries continue to get vaccines (and booster shots) first but neglect to accelerate production sufficiently to cover poorer nations in time to prevent mutations is both patently unfair and self-destructive. We are in a race against time, and the costs of accelerating global vaccine production are measured in the billions whereas the benefits of reaching global immunity a few months earlier are measured in the trillions.
The World Health Organization and pharmaceutical companies have responded to this situation through the creation of COVAX, a pool of pledged vaccines specifically to help vaccinate low-income nations. This is an important program and the recent Biden investment of 4 billion dollars to the fund should be applauded. But the scope is still lacking in the necessary ambition. The aim of the program is to supply vaccines to help participating counties vaccinate only 20% of their population.
Ultimately, we need to be producing more vaccines in less time. One way of achieving that is to make it easier for competing vaccine manufacturers to get in on the action. Specifically, if there is latent vaccine manufacturing capacity (more on this controversial point later), we could pull out all the stops by suspending the intellectual property protections. This should help speed the vaccination efforts around the world, and if the latent manufacturing capacity is located in the Global South, it could make the future waves of vaccine booster shots more equitably distributed given the apparent home-market bias of current producers.
This last point connects to a larger question around self-sufficiency and national sovereignty in vaccine and pharmaceutical production. Much of this conversation is informed by the context of the HIV/AIDS epidemic of the 1990s to early 2000s which ravaged countries across Africa while the US and other wealthy nations were able to mitigate the damage using antiretroviral treatments. A combination of strict IP enforcement, a lack of foreign aid, and inadequate manufacturing capacity lead to millions of deaths that potentially could have been prevented. In 2003, the US created PEPFAR, an extremely successful public health campaign that was able to make massive dents in the crisis by sharing medicine and technical support with partner countries. To counter the concern that IP issues would hamstring future public health responses, the WTO signed the Doha Declaration which created rules around compulsory licensing of medical technology in the event of a public health emergency (but which advocates say are insufficient for this present situation). Given this history, developing nations are understandably skeptical of the idea that they should wait around for Western pharmaceutical companies to produce enough vaccines for them and would like to develop their own manufacturing capacity.
Finally, advocates for suspension typically point out that many of the pharmaceutical companies received R&D funding from the federal government and/or large market commitments through Operation Warp Speed, which guaranteed them some baseline level of confidence and profitability. Furthermore, the mRNA vaccines themselves are partially the result of decades of public investment in science, and indeed the National Institutes of Health may own some parts of the relevant IP in the case of Moderna. If you are inclined to believe that pharma R&D is mostly free-riding on the hard work of basic science, then this is a pretty clear-cut case for suspending the IP.
In short, we’re not safe from Covid until we are all safe. So let’s tear down any red tape or barriers that may be slowing the production and deployment of vaccines around the world.
The case against suspension:
On the anti-suspension side, there is the argument that these new vaccines (especially the new mRNA vaccines) required billions of dollars and decades of uncertain private investment to reach the technical breakthroughs that have given us a chance to end this pandemic. Yes, basic science work funded by the government helped a lot and established a strong foundation for much of this work. But enterprising individuals with a profit motive played just as large a role. Katalin Karikó, the Hungarian scientist who helped pioneer mRNA vaccines spent most of the 1990s receiving rejection letters for government grants and ultimately turned to the private sector where she co-founded her own company in 2006.
But even if all the basic research were federally funded, the argument for suspension would still create incentive issues. Operationalization and commercialization of scientific breakthroughs are essential and still cost a lot of money. There are a whole series of difficult engineering, logistics, and optimization problems that have to be solved when taking a complex biological product like a vaccine from research to reality. They do not pop out into the world fully formed from a peer-reviewed publication in Science. And it’s no accident that the countries with the most well-developed biotechnology and pharmaceutical clusters are the ones that produced these wonders.
Where most public health interventions failed miserably, the pharmaceutical companies worked around the clock to develop, test, and roll out a whole new genre of vaccine in record-breaking time and at high private cost. To expropriate the intellectual property that makes the whole investment pipeline worth it in the first place is to place future R&D investments under a great shadow. This is, unfortunately, unlikely to be the last global pandemic we face. And we got lucky that Covid-19 has a relatively low fatality rate and that we were able to so easily target its spike protein. To ensure that our biotechnology clusters are investing in R&D for new vaccine and therapeutic techniques for the future, we have to align incentives and make it profitable for them to throw billions of dollars at the problem years before it may ever appear.
Furthermore, all the focus on intellectual property conceals the point that the formalized information that can be written in a patent application isn’t that useful in isolation. Moderna actually pledged in October that they would not be enforcing the IP rights related to their Covid vaccine. And the underlying spike-encoding sequence was recently published online by Stanford researchers. However, no new Moderna knock-offs have sprung up since their October announcement. Why? Because the company has refrained from sharing any details about the manufacturing or design process, which indicates the underlying technical expertise and production process knowledge are just as important.
As Rachel Silverman from the Center for Global Development notes:
Observing their contents is insufficient to allow for imitation. Instead, to produce the vaccine, manufacturers need access to the developer’s “soft” IP — the proprietary recipe, cell lines, manufacturing processes and so forth. While some of this information is confidentially submitted to regulators and might theoretically be released in an extraordinary situation (though not without legal challenge), manufacturers are at an enormous disadvantage without the originator’s cooperation to help them set up their process and kick-start production. Even with the nonconsensual release of the soft IP held by the regulator, the process of trial and error would cause long delays in a best-case scenario. Most likely, the effort would end in expensive failure.
Typically this kind of soft IP is transmitted to the new company in a technology transfer process that happens during a licensing deal. Process experts from the licensing firm will sometimes travel to the facilities of the licensee and oversee operations for the first several batches to help convey the sort of tacit knowledge that is difficult to transmit unless you have physically done the operation yourself. In exchange, the licensing company will get a cut of the revenue from each dose, typically 5-10%. However, even when these licensing deals are in place, it’s easy for the new firm to make critical mistakes because the margins for error are razor-thin.
All this means that if the TRIPS proposal were passed in isolation, it would likely lead to little appreciable change in vaccine production unless it was paired with significant incentives for the manufacturers to play ball on the more formalized technology transfer process.
The open question: is there latent capacity?
Does this mean we are already at the frontier of vaccine production and there’s nothing more to be done? I doubt it.
In some sense, the easiest thing to do would be to plow many billions more into programs like COVAX, which reserves vaccine doses for developing nations. That would be good, but it may just extend the length of vaccine production rather than increase the rate of production. Maybe we could specifically help pay for existing vaccine manufacturers to scale up their capacity even more? This too, would be worthwhile. After all, it’s difficult to imagine having too much vaccine capacity (from a social welfare perspective). But even here, building new factories and machines can take months or years, and it would be nice to have something that works more quickly. Secondarily, this solution will only continue to concentrate vaccine production in existing firms and in rich nations, which undermines the self-sufficiency concern that helped fuel this debate.
The main advantage that some version of IP suspension offers is activating manufacturing capacity that already exists but isn’t currently being deployed. But how much latent capacity is there actually?
Especially for the mRNA vaccines of Pfizer and Moderna, it appears that the production bottlenecks are quite severe. A great piece by Derek Lowe outlines how specialized the supply chains and manufacturing processes for mRNA vaccines are, especially in their use of lipid nanoparticles. Lowe argues that only a handful of firms globally could have jumped in and started making mRNA vaccines immediately, and it seems likely that all of them already have.
However, this may be too fatalistic about the supply elasticity over a slightly longer time horizon. Production bottlenecks can ease over time with enough investment and learning by doing. Due to the massive social and economic costs we face during each additional day of this pandemic, even a slight increase in production can justify a significant price tag.
It seems more plausible, however, [I have no special expertise in vaccine manufacturing, so take this for what you will] that there is latent capacity using the more traditional adenoviral vector vaccines like Johnson & Johnson and AstraZeneca. Because adenoviral vector vaccines have the advantage of having simply existed for longer, more vaccine manufacturers around the world have the capacity to produce them than can produce mRNA vaccines right now. The related supply chains are more mature as well, which means a sudden surge in demand can be better accommodated. We saw this play out with the Serum Institute of India, the world’s largest vaccine manufacturer, which opted to take a voluntary licensing deal to manufacture the AstraZeneca vaccine at scale.
There may also exist capacity that is not exactly latent, but is not being used very efficiently. If an opportunity presented itself, we could see some vaccine manufacturers who are currently pursuing vaccine trials that will otherwise be late to the game drop their research trials and focus on producing known (and already approved) vaccines. Sanofi and GlaxoSmithKline, for example, began a phase 2 clinical trial in February that (if everything goes right) will finally be ready in Q4 of this year. There’s no particular reason to think this new vaccine will be better than the existing offerings. It’s more likely that they are pursuing this line because they know the vaccine rollout around the world will be slow and they want to have proprietary IP to offer. While both Sanofi and GSK have signed deals to help manufacture other vaccines in the meantime, these are quite limited and the companies are likely saving capacity so they can rapidly retool if their own trials are promising. But it would certainly be more socially valuable if we could encourage them to drop these trials and fully ramp up the production of proven vaccines right now. There are also companies like Merck that appear to be mostly sitting out the Covid vaccine rush altogether after their own efforts failed.
The case for buyouts:
The economist Michael Kremer wrote a paper in 1997 formalizing the idea of using patent buyouts as a way of maintaining strong incentives for innovation while still getting crucial information into the public domain ASAP. Essentially, a government could offer to pay the present value of the expected future revenue stream that would result from the temporary monopoly that a patent grants. While the patent-owning company or individual should be indifferent to the outcome, the general public could receive more value from having unabridged access to the information and the ability to modify it without permission before the patent expired. In these cases, a patent buyout can clearly improve outcomes for everyone, and Kremer notes that pharmaceuticals may be a particularly appropriate case.
Patent buyouts present at least a theoretical solution to the problem of maximizing the number of players that can legally produce vaccines while maintaining strong incentives for innovation in the future. Of course, in this situation it’s only partly about the intellectual property and partly about the manufacturing know-how that has to be transferred, which means we need a broader conception here — a full stack “technology buyout” which includes both the IP and the promise to transfer process knowledge.
Essentially, the US government (or conceivably a set of governments, but that would take longer to negotiate) could offer a lump sum payment to the accepting firm or firms to write down as much about the scientific and production process as can be made explicit and then make it publicly available. There could then be additional payments made for the sharing of tacit knowledge and aid in setting up the manufacturing operations either on an individual factory level, or on a per vaccine dose administered basis. The advantage of additional payments of a per vaccine dose administered basis is that it properly aligns incentives for the firm(s) sharing technology to maximize their impact by transferring to partners that can actually get shots into arms as quickly as possible and to make sure they do a good job.
To make this concrete and put some back-of-the-envelope numbers on this, I would suggest the initial lump sum payment to make the IP public would be in the range of $10-20 billion, and the additional per dose administered prize would be in the realm of $0.50 – $2. Assuming this program was able to administer vaccines for an additional 4 billion people (8 billion doses) across the developing world, we are talking in the range of $36 billion dollars.
And we should in some sense actively try to overpay. In unique situations like this, we should err on the side of overcompensating and risking some economic rents rather than inadvertently under compensating and hurting the long-term incentives for innovation. The most important thing here is that we do not kill the goose that lays the golden egg. In any event, we should be willing to pay an order of magnitude more than $36 billion to definitively end Covid, so this program should be a bargain under a wide range of potential cost assumptions. One estimate from a group of economists and public health officials ballparks the global cost of the pandemic at around $1 trillion per month.
Some readers may note that “payments for each vaccine dose administered” sounds very similar to the voluntary licensing agreements that manufacturers around the world have already signed. And they are correct, it’s a closely related mechanism. Indeed, commentators like Rachel Silverman (quoted above) have actually suggested that the best way forward may be having the federal government use its political leverage to lean on US pharmaceutical companies to accept more licensing deals with manufacturers in developing countries. Which raises the question, why bother doing the additional lump sum buyout to make the information public? Shouldn’t we concentrate all our efforts on encouraging licensing?
I would differentiate the technology buyout I’m suggesting from voluntary licensing on a few dimensions:
First, buying out the IP may be a determining factor for encouraging large, mature manufacturers like GSK and Sanofi to abandon their own duplicative vaccine trials and go full steam towards producing existing vaccines as it removes any competitive disadvantage in paying the licensing fee.
Second, because these voluntary licensing deals are typically assigned as a percentage of the dose cost, it creates an incentive for licensing firms to prioritize deals that will charge a higher price to the buying local governments where this may not be optimal. If the US government is instead paying for each dose administered in these developing nations, then the transferring firm(s) should be neutral with regard to the sale price.
Third, this structure allows the federal government to selectively overpay on a per dose basis if the US firm is genuinely helping a developing nation jumpstart new manufacturing capacity as opposed to helping an existing manufacturer retool.
Fourth, individual countries and foreign manufacturers know better their own capacity than US government officials or even US firms do, so opening up the IP could help identify latent manufacturing opportunities more effectively than a top down approach.
Fifth, opening up the IP at least gives every nation the ability to try and make their own vaccine if they so wish, which helps address the self-sufficiency concerns.
A buyout also presents several key advantages when compared to IP suspension as well, even putting the incentive issues aside.
First, speed. Even if the US were to reverse course and support the WTO proposal, it would take quite a bit of time to negotiate and wrangle all the other countries to the table. Remember, the proposal has to be supported unanimously, so there is no guarantee that the EU, UK, Australia, and other opposed nations will reverse course just because the US does. A buyout, in contrast, can be done unilaterally by the US (at least for the US based vaccine firms).
Second, in the unfortunate event that a new variant of Covid requires a booster shot, a buyout ensures the incentive to quickly create a solution (so that the new booster shot can also get bought out). Under the WTO petition, the IP suspension would remain in play for the duration of the crisis, which would reduce the urgency and resources that pharma companies are willing to throw at the problem, given fewer opportunities to recoup costs.
Building for the long term
Finally, there is the issue of whether a technology buyout would be better suited for the mRNA vaccines of Modena and Pfizer or for an adenoviral vector vaccine like Johnson & Johnson. To answer that we have to ask a more fundamental question: what is it we are trying to achieve here? There is likely more short term capacity to scale adenoviral vector vaccines, so if we are narrowly trying to get the world vaccinated against Covid-19 as quickly as humanly possible, then a technology buyout for the J&J vaccine probably makes the most sense.
But if we have a larger vision of using this crisis as an opportunity to bootstrap new, flexible vaccine manufacturing capacity around the world for the future, then mRNA vaccines have a host of advantages that will make them the better long-term pick. Of course, we can try to do both to take advantage of the distinct advantages of each vaccine type, but it helps to have a longer term anchor goal to build towards.
A few points in favor of the future oriented approach. First, hoping the adenoviral vector vaccines hold up long enough against possible variants is a significant risk. As alluded to earlier, the mRNA vaccines appear to be more resilient to the recent Covid variants and are significantly easier to modify in the event a new variant arrives that our current vaccines can’t handle.
Second, there have been a series of exciting news developments in the last few months indicating that mRNA vaccines could unlock a much broader wave of medical improvements, including possible vaccines for multiple sclerosis, some forms of cancer, malaria, and HIV. All of which means mRNA is likely to be a more general purpose vaccine technology and makes it almost impossible to imagine having overbuilt capacity at this point.
Third, separate from the supply chain issues, new mRNA facilities are actually much cheaper to build and operate than traditional vaccine factories. From an article in the Journal of Advanced Manufacturing and Processing:
Based on our techno‐economic assessment, the RNA vaccine production process can be two to three orders of magnitude smaller than conventional vaccine production processes in terms of facility scale, and can be constructed in less than half the time with 1/20 to 1/35 of the upfront capital investment… It therefore presents a strong advantage of requiring small‐scale, high‐capacity facilities, which can be constructed more rapidly and could make wide use of single‐use disposable equipment. Due to its small scale, the RNA vaccine drug substance production process could be placed in a small part of an existing conventional vaccine facility, for example in a room, and still produce more doses worth of drug substance than the entire original conventional vaccine production facility.
Fourth, we should view this as an opportunity to build good will around the developing world. The total US foreign aid budget was around $40 billion in 2019, right in the range of what we are proposing here. I’m inclined to believe sharing new, highly effective technology around the world during this unique crisis would generate a significantly higher return diplomatically than the projects we usually get with this scale of funds. Already we’ve seen China and Russia attempt to leverage their vaccine exports for diplomatic purposes. Indeed, another lens you could use for this would be as a kind of liberal counter-weight to the Belt and Road initiative that has helped China make inroads across Africa. Instead of physical infrastructure investment, the US would be helping them with technological infrastructure investment.
Finally, it is in the long-term interest of all of humanity to have a developed and coordinated ability to respond to new diseases around the world. Viruses don’t respect national borders and the risk of a global pandemic has only increased over time as our world has become more interconnected. This capacity inherently needs to be distributed around the world for it to be maximally effective, so we may as well start building it out now. On the high-end of effectiveness, this capacity to rapidly create and distribute new mRNA vaccines could help us eliminate much of the long term risk of bioweapons and natural pandemics. That is the true goal worth aspiring toward here.
Conclusion
The world needs more vaccines and we need them quickly. It seems unlikely that suspending the IP rights will do much to accelerate production in isolation and it could significantly diminish the incentives for investing in the future. On the other hand, a full technology buyout — which includes the IP rights and incentives to work with foreign manufacturers — could simultaneously activate any latent capacity that may exist while also giving the developing world an opportunity to bootstrap their own vaccine manufacturing capabilities with the help of American know-how.
The US should be aiming not only to vaccinate the entire world, but to teach the world how to make vaccines. As the famous saying goes: give the world vaccines and you stop one pandemic, teach the world how to manufacture mRNA vaccines and you stop pandemics forever.
Bera: It doesn’t do us any good if you give someone health insurance coverage, but you can’t afford to use it.
On this week’s PPI Podcast, Arielle Kane, PPI’s Director of Health Care sits down with Rep. Ami Bera, M.D. (CA-7), a leader of the New Democrat Coalition. They discuss National Public Health Week, the critical funding within the American Rescue Plan Act, and the state of health care after the COVID-19 pandemic.
“We’ve got to do a better job providing services and managing the health of those 20 percent [of Americans] with chronic conditions to both better manage their disease but also prevent some of those conditions. I think if we’re able to do some of that – and that’s something the New Democrat Coalition has worked on through various venues – we can start to bend the cost curve down,” said Rep. Ami Bera on the podcast.
Representative Bera also discussed the intersection of health care and infrastructure, and the work Congress and the Biden Administration is doing to improve access to care for all Americans:
“We’ve seen with the pandemic things like telehealth, telemedicine, have really been impactful in helping care for patients who may not have wanted to leave their home – and rightfully so – in the middle of a pandemic. That’s something that we should keep in place. But you can’t do telemedicine or telehealth if you don’t have broadband access – or it’s very hard to do. So let’s get that access out to those communities. That will help us solve some of the issues of lack of specialty care if you’re in a small rural community…” said Rep. Bera.
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
On this week’s PPI Podcast, Arielle Kane, PPI’s Director of Health Care sits down with Rep. Ami Bera (CA-7), a leader of the New Democrat Coalition. They discuss National Public Health Week, the critical funding within the American Rescue Plan Act, and the state of health care after the COVID-19 pandemic. Representative Bera also discussed the intersection of health care and infrastructure, and the work Congress and the Biden Administration is doing to improve access to care for all Americans.