Is the coronavirus about to force us into the Biotech Century? Here’s a follow-up to my previous post.
In response to the coronavirus pandemic, government and private researchers are taking the perhaps unprecedented step of testing the safety of a new coronavirus vaccine in volunteers before testing its safety and efficacy in animals. As one researcher told STAT, a medical news publication:
“This is very unusual,” explained Akiko Iwasaki, a Yale University microbiologist who studies the immune response to viruses. “It reflects the urgency to develop vaccines to counter the Covid-19 pandemic.”
This experiment in accelerated science could fail in two ways. First, the vaccine could turn out to be unsafe or ineffective in the volunteers. That’s not at all unlikely. This particular vaccine is being developed by a new methodology from Moderna. Unfortunately, as the New York Times wrote, “no vaccine made with this technology has yet reached the market.”
The second way that the new vaccine could fail is that it could look safe and effective in clinical trials, be put into widespread use, and then show unforeseen side effects. That could be medically and scientifically devastating, and it can’t be ruled out either. As STAT notes, medical ethicists are conflicted about the wisdom of accelerated science.
The upside, though, is potentially enormous. A vaccine against COVID-19, even one that is only partially effective, could spare millions of people from dying worldwide, while allowing the global economy to be reactivated.
This vaccine trial is not alone. Accelerated science is going on at all these tests of new coronavirus treatments and vaccines going on all around the globe. Academic researchers, companies and government regulators are willing to throw normal procedure aside because the stakes are so high.
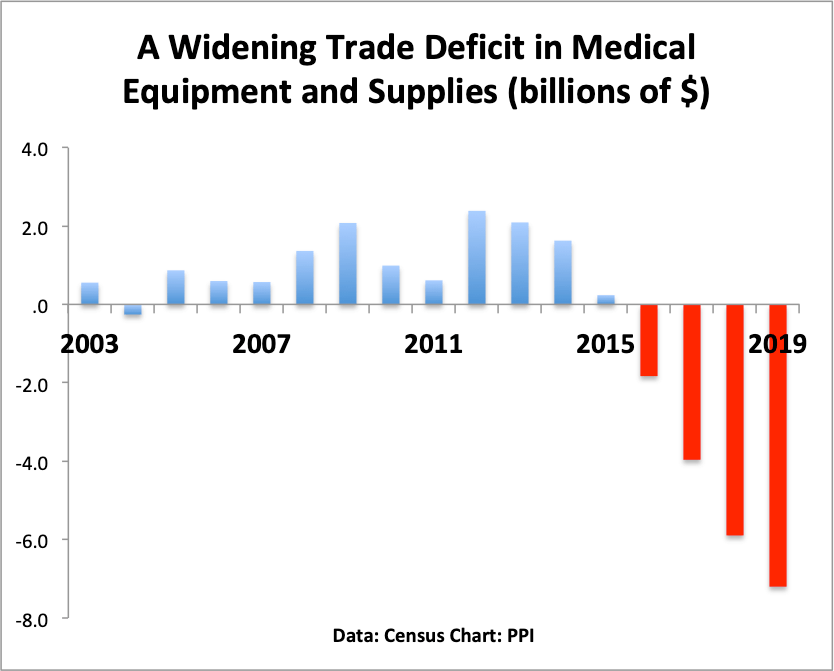
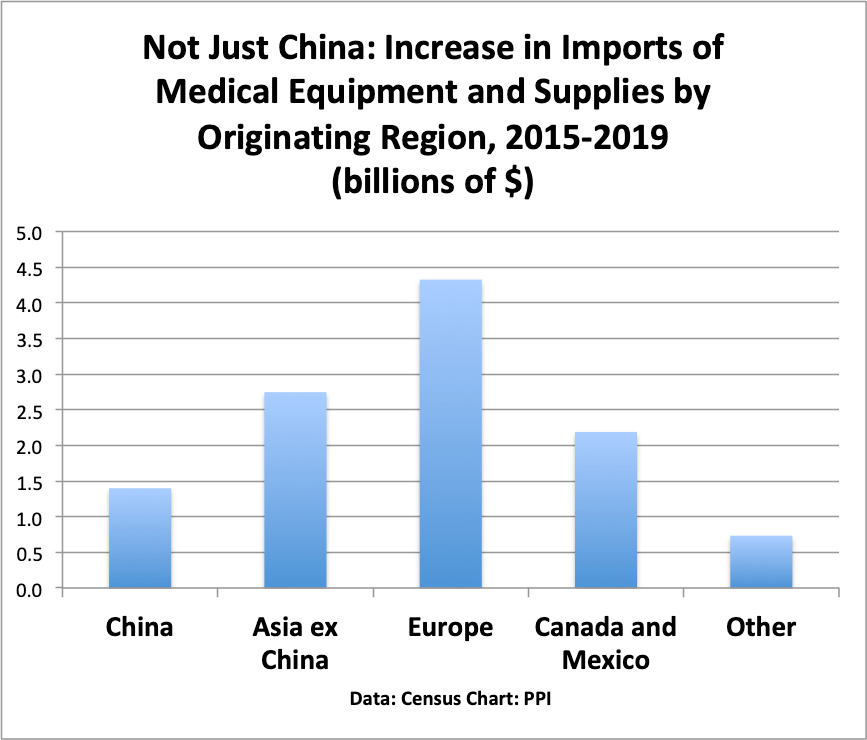
As these tests proceed, we will also learn something important about progress and innovation. As noted here, we’ve spent close to $2 trillion on biosciences research and development over the past 25 years, and we haven’t gotten the payoff in better health or economic growth that we expected.
One possibility is that well-intentioned government regulation systematically impeded disruptive innovation in the biosciences, as I argued my 2014 essay “Hacking the Regulatory State” and my 2011 policy brief on medical innovation. It wasn’t malicious, but as I wrote:
A disruptive innovation, as identified by Clayton Christensen, starts out as less capable than existing technologies, but as the innovation evolves, it gets both cheaper and more powerful.
The first automobiles, for example, were both more expensive and less reliable than a horse. Similarly, the first personal computers were basically toys compared to the existing minicomputers and mainframes. But they got better and cheaper over time.
From that perspective, it’s clear that a government regulatory body with “too-high standards” can have the effect of choking off innovation. Imagine how the history of computing would have been different if Steve Jobs and Steve Wozniak had to prove that the Apple I could meet government performance standards before it could be sold.
FDA standards require both safety and efficacy, meaning that the drug or medical device have to perform better or at a minimum just as well as existing alternatives.
It’s important to note that the first personal computers would not have met FDA-type efficacy standards, and neither would have the first cell phones. When cell phones were first introduced in the 1980s, they were bulky, heavy devices which retailed for $4000, provided terrible reception and could barely fit in a briefcase, much less a pocket. By any measure, they were inferior in phone quality to existing wireline services. Today, most people have given up their wirelines in favor of mobile devices.
Under ordinary circumstances, it makes sense to apply tighter standards to medical innovation than to IT innovation. Under ordinary circumstances, people want assurances that a new drug or medical device is safe, and will work at least as well as the alternative.
These are not ordinary circumstances. The tragedy of the coronavirus pandemic is forcing us to try things and make decisions that we would never do in the normal course of affairs. We are in uncharted territory, and there are no guarantees. We could learn that the regulators were right, and disruptive innovation is the wrong model for medical science. Or we could learn that medical science has advanced far enough to produce vaccines and treatments for new diseases in far less time than normal. And that would be the dawn of the Biotech Century.