This post begins our series on “The Next Ten Million Jobs.” Based on our analysis of the latest BLS employment projections, the U.S. economy will produce roughly 10 million jobs between now and 2030. The question is what kind of jobs will they be; how can Americans prepare for emerging new occupations; and what can policymakers do to improve the job situation.
We use the BLS projections as a starting point, but we don’t take them as gospel. First, we extend them from 2028 to 2030, to actually give us a ten-year projection horizon for the presidential race of 2020. But we also dig deep into some of the assumptions underlying the official projections. In particular, they can be thought as embodying a cautious extrapolation of current technological trends. For example, the BLS expects the number of heavy and tractor-trailer drivers to grow over the projection horizon, rather than being suddenly wiped out by autonomous trucks.
But recent history shows that technological change can drive sudden shifts in jobs, and create emerging new occupations. For example, the rise of ecommerce fulfillment centers means that the number of workers employed in the warehousing industry grew much faster than expected. Based on the BLS projections released in 2009, the warehousing industry was only expected to add 80K jobs between 2008 and 2018. Instead, the actual gain was closer to 500K.
Similarly, in 2007 no one could have predicted the rise of the App Economy, which has created so many new jobs since the introduction of the iPhone and all the smartphones to follow. Our latest estimate shows that the U.S. has roughly 2.2 million App Economy jobs, including a conservative calculation of spillover jobs. These jobs are supported by a bevy of technologies, including the iOS and Android mobile operating systems and the related app stores; fast and extensive mobile networks, which operators such as AT&T and Verizon are spending billions to upgrade to 5G; and an incredible number of mobile applications for consumers and businesses, written and maintained by both small app developers and app developers working for large companies.
In this series of posts we’re going to try to identify some emerging new occupations and industries that have the potential to create new job opportunities for Americans. These may or may not correspond to the BLS projections.
But for this first post, we start with the single biggest headline from the BLS projections: The importance of healthcare and social assistance jobs for the labor market. By our estimate, out of 10 million net new jobs by 2030, more than 4 million will be in healthcare and social assistance. As a result, between now and 2030, growth of healthcare and social assistance jobs accounts for 44% of the net growth of nonagricultural wage and salary jobs. That’s up from 39% in the period from 2007 to 2018.
In effect, healthcare has become the black hole of the labor market, sucking in workers at a prodigious rate.
From the perspective of young people entering the labor market, these huge numbers send a clear signal that healthcare is the place to be. Why wouldn’t you aim for the industry that is creating almost half of new jobs?
The problem for policymakers, though, is that the rapid growth of health care jobs is the single biggest driver of healthcare spending increases, as we have noted in past posts, by a wide margin. So the only way to restrain healthcare spending is to hold down health care job growth.
This takes on special meaning as proponents of various healthcare reforms try to find a way to hold down costs to make the numbers works. In this context, it should also be said that many European countries, with different health care systems than ours, are seeing an equally rapid growth in healthcare and social assistance jobs. For example, in Germany, health and social assistance jobs amounted to 37% of net new jobs created between 2008 (the business cycle peak) and 2017, the last data available. That’s based on OECD data.
Going forward, we can imagine two alternative scenarios to the BLS healthcare employment projections. In one scenario, a Democratic victory in 202o leads to expanded healthcare coverage, either in the private sector or by offering a public option. In that case, the number of jobs will increase faster than expected, and young people who go into health care will find a very strong labor market.
In the other scenario, policymakers try to hold down the growth of healthcare costs by boosting labor productivity and restraining the growth rate of health care jobs. That means young people who go into health care run the risk that health care job growth will be less than expected.
A new report from the Congressional Budget Office projects federal budget deficits between 2019 and 2029 to be $872 billion higher than was projected just three months ago. As a result, Donald Trump will be forced to campaign for re-election next year with his government running a trillion-dollar deficit. Democrats should hold the “king of debt” accountable for his inability to manage the nation’s finances and present voters with a compelling alternative: a new progressivism that invests in our country without burying young Americans under a mountain of debt.
The increase in CBO’s deficit projections is largely due to the bipartisan budget deal signed into law this month and other spending policies enacted over the summer, which CBO says together will cost nearly $2 trillion – making them almost as expensive as the tax-cut bill enacted by Trump and the Republican-controlled Congress in 2017. Projected deficits also increased by almost $280 due to technical changes in CBO’s modeling. Partially offsetting these costs was a reduction in CBO’s forecast for interest rates, which brought projected deficits down by a whopping $1.4 trillion.
That a change of less than one percentage point in interest rates can cost nearly as much as the budget deal or the Trump tax cuts is a testament to the size of our national debt on which that interest is owed. The $16.5 trillion debt (which grows to almost $22.5 trillion if one includes intragovernmental debt such as that owed to the Social Security and Medicare Trust Funds) will only become worse moving forward as the government is projected to spend $1 trillion more than it raises in revenue every single year from 2020 onward if current laws remain unchanged.
While the left and center-left have been debating the wisdom of abolishing private insurance, another critical policy issue has not gotten much attention: The Medicare-for-all bill currently in question would create a single-payer health care system based on fee-for-service, disregarding the financial and outcome-based successes of Accountable Care Organizations, the Center for Medicare and Medicaid Innovation (CMMI), Medicare Advantage, and other payment reforms emphasizing value-based care.
Cigarette smoking by Americans declined steadily from the mid-1960s to around 2005, when this progress began to slow. From 2013 to 2017, however, cigarette smoking rates fell sharply, during a period in which the use of electronic cigarettes or e-cigarettes increased sharply. This study examines the connection between these two developments and the implications.
Among adults, cigarette smoking rates fell from 18.0% in 2013 to 14.0% in 2017, while the use of e-cigarettes increased from 1.9% to 2.8%.
Over the same years, cigarette smoking rates among high school students fell from 12.7% to 7.6% while their rates of e-cigarette use increased from 4.5% to 11.7%. Among adolescents, the association between declining smoking rates and rising e-cigarette use was even stronger than among adults.
Statistical analysis of the changes in smoking rates and e-cigarette use by age, gender, race and ethnicity suggests that about 70 percent of the increased decline in cigarette smoking from 2013 to 2017 was associated with the rising use of e-cigarettes. The remaining 30 percent was associated with higher cigarette taxes, bans on cigarette sales by the CVS pharmacy chain, and increased use of anti-smoking prescription drugs.
Statistical analysis also strongly suggests that e-cigarettes are not a gateway to smoking cigarettes.
Rather, statistical analysis and numerous studies establish that e-cigarettes are an effective tool to help people stop smoking or avoid starting to smoke cigarettes.
Based on these analyses, we estimate that pre-existing trends and factors other than e-cigarettes can explain a decline in smoking rates by people ages 18 to 44 from 20.2% in 2014 to 17.9% in 2017. However, the rate fell from 20.2% to 14.6% in 2017, and the rising use of e-cigarettes can explain the additional 3.3 percentage-point decline in cigarette smoking rates.
By this account, e-cigarette use is closely linked to a reduction in cigarette smoking from 2014 to 2017 by 922,301 people ages 18 to 24 and 2,922,540 people users ages 25 to 44, or a total of 3,844,840 people.
We also calculated the healthcare savings and costs and the productivity benefits associated with the reductions in cigarette smoking and the increased use of e-cigarettes from 2014 to 2017 by those 3,844,840 people ages 18 to 44. These calculations are based on healthcare costs, life expectancy, and the differences in the incidence of illnesses that interfere with work for smokers, ex-smokers, nonsmokers and e-cigarette users.
E-cigarette use lowers people’s annual per capita healthcare costs, compared to cigarette smokers and ex-smokers, for all age groups up to age 75.
For people ages 25 to 44, the annual per capita healthcare costs of cigarette smokers are 9.8 percent greater than those of e-cigarette users, and the average annual per capita healthcare costs for ex-smokers are 19.8 percent greater than for e-cigarette users.
For people ages 45 to 64, annual per capita healthcare spending for cigarette smokers is 8.8 percent greater than for e-cigarette users, and average per capita healthcare costs for ex-smokers are 34.4 percent greater than for e-cigarette users.
Treating cigarette-smoking-related diseases accounts for an estimated 8.7 percent of annual healthcare spending, or $303.8 billion in 2017.
By reducing the number of people who smoke cigarettes, e-cigarette use also extends the lifespans of millions of people, raising their lifetime medical costs across all age groups except those 18 to 24.
We calculate that the use of e-cigarettes by the 922,301 people ages 18 to 24 in 2017, who otherwise would have started smoking cigarettes, should reduce their lifetime healthcare costs by $11.3 billion.
However, the use of e-cigarettes by the 2,922,540 people ages 25 to 44 in 2017,
who otherwise would have started smoking cigarettes, increases their lifetime healthcare costs by $284.5 billion.
Those higher lifetime healthcare costs reflect spending for 330,489 people whom we would expect to have died before their mid-to-late 60s if they started smoking cigarettes in 2014- 2017, and for 500,865 people whom we would expect to have died before their mid-to-late 80s if they had started smoking instead of using e-cigarettes.
E-cigarette users (and nonsmokers) also are more productive than smokers, because smokers miss more work due to illness, come to work still impaired by illness more often, and take smoking breaks. We found that e-cigarette users are on average $820 more productive per-year than ex-cigarette smokers and $2,371 more productive per-year than current smokers, and that ex-smokers who shifted to e-cigarettes are on average $1,554 more productive per-year than current smokers.
The additional productivity of the share of the 922,301 e-cigarette users ages 18 to 24 in 2017 who worked from 2017 on, and who otherwise would have become smokers in 2014-2017, would be worth $14.7 billion over the 10 years from 2017 to 2027;
The additional productivity of the share of the 2,922,540 e-cigarette users ages 25 to 44 in 2017 who worked from 2017 on, and who otherwise would have continued to smoke in 2014-2017, would be worth $29.2 billion over the years from 2017 to 2027.
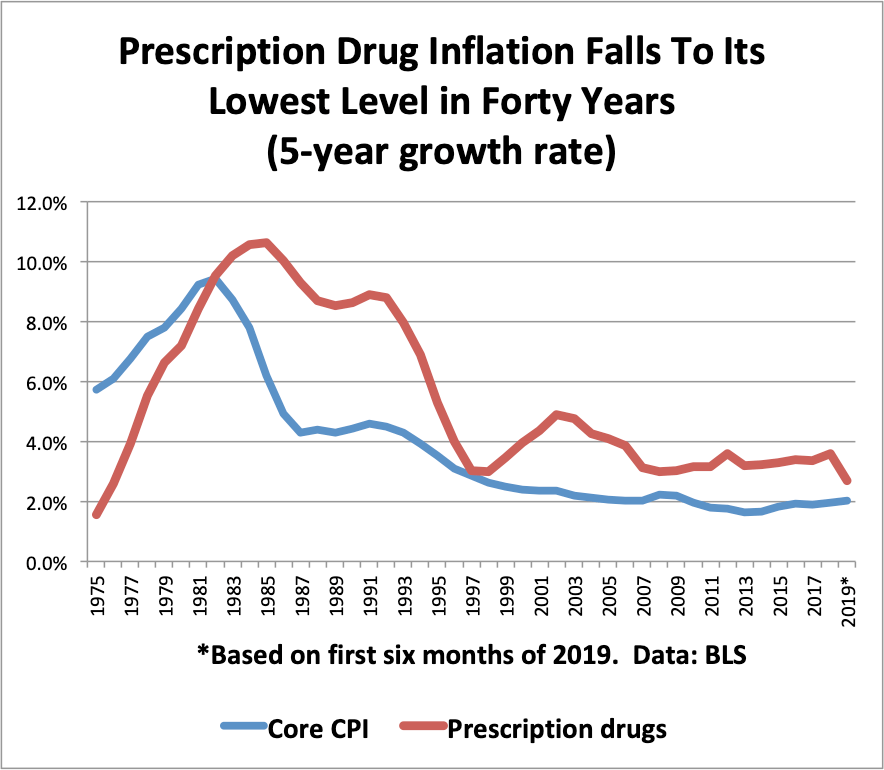
In the first half of 2019, the consumer price index for prescription drugs fell by 0.8% compared to the first half of 2018. That’s the first year-over-year decline in prescription drug prices since the mid-1970s, according to BLS data.
Looking at five-year inflation rates, the consumer price index for prescription drugs rose at a 2.7% rate from 2014 to 2019, based on the first six months of this year (see chart below). This represents the slowest rate of prescription drug inflation in forty years, according to BLS data.
We also note that prescription drug inflation is now only slightly above core CPI inflation, which is running at a 2.0% pace from 2014-2019.
That doesn’t let the pharma industry off the hook for the behavior of bad actors, especially as we learn more about the opioid epidemic. But it does suggest that the problem of drug pricing may be a bit more complicated than it seems.
The Progressive Policy Institute’s Health Care 2020 panel relayed the overwhelming opinion that the American health care system is broken and in desperate need of reform.
Americans need health care reform to achieve timely access to effective, affordable, and quality medical care. The Progressive Policy Institute (PPI) hosted a panel discussion on Wednesday, July 24th featuring the Honorable John Kitzhaber, MD, Tara O’Neill Hayes, Anand Parekh, MD, and Arielle Kane on the often forgotten elements of comprehensive health care reform.
The panelists discussed how to get to universal coverage, how to transition to an accountable delivery system, the need for a global budget, and, most importantly, how to reinvest savings to address social determinants of health. Governor Kitzhaber said that “at 18 percent of GDP, we know that health care has huge opportunity costs. When you look at the things that have long term impacts on health, it’s housing, safe communities, maternal care, and other social determinants of health.”
This conversation, with over 80 people in attendance, focused on crucial elements of holistic health reform rather than the more frequent discussions around “repeal-and-replace” or “Medicare-for-all.” Anand Parekh, MD, MPH, the chief medical advisor of the Bipartisan Policy Center noted that: “A lot of the oxygen in the debate surrounds increasing access to affordable health insurance and access to affordable prescription drugs. Those are critical — but it’s also important to focus on what happens beyond the four walls of a health center.” This focus on health beyond the hospital included a discussion of preventative care and improving health in a financially sustainable way.
Tara O’Neill Hayes, the deputy director of Health Care Policy at the American Action Forum, said “Medicare and Medicaid already account for 26.5 percent of the federal budget, with a percentage that’s grown each year. By 2027, these two programs alone will cost the federal government over $2 trillion.”
The overwhelming sentiment was that the American health care system is broken and in desperate need of reform in a manner that is both financially sustainable and prioritizes patient outcomes.
“Health care and poverty are inseparable issues and no program to improve the nation’s health will be effective unless we understand the conditions of injustice which underlie disease. It is illusory to think that we can cure a sickly child and ignore his need for enough food to eat.” Robert Kennedy, 1968
Reframing the 2020 Health Care Debate by the Honorable John A Kitzhaber, M.D.
Last month’s Democratic debates demonstrate how central health care will be in the 2020 election. Indeed, health care, more than any other issue, propelled the Democrats to regain control of the House of Representatives in 2018. Whether the upcoming election leads to meaningful relief for the millions of families struggling under the escalating financial burden of medical care, however, depends largely on how the issue is framed and on the clarity with which we see our policy goal and the steps necessary to achieve it.
Today the vast majority of dollars in our health care system are spent on the after-the-fact treatment of acute and chronic medical conditions rather than on investments that could prevent these conditions in the first place.
If we could reduce our health care spending from the current 18 percent of the GDP to the 12 percent average of most other industrialized nations, it would free up well over a trillion dollars a year for the social investments that actually improve health (1).
What concerns voters most about health care and, by a wide margin, is the cost — but, and this is important — not the cost of the overall U.S. health care system, but the cost to them as individuals (2). Most voters believe, to some extent in the abstract, that everyone should have access to affordable health care, but they are far more concerned that they as individuals have access to affordable health care. This is understandable because, at the end of the day, health care is intensely personal.
And yet, it is fair to say that nobody wants to need medical care or to be a “patient.” When you are sick or injured it is important that you have timely access to care at a cost you can afford, but we also know that among the factors contributing most to lifetime health status, our medical system is a relatively minor contributor. Far more important are things like healthy pregnancies, affordable housing, nutrition, stable families, good jobs, safe communities and the other “social determinants of health” (3),(4).
Therefore, our policy goal should be to improve the health of our people through a system that is financially stable, ensures that all Americans have timely access to effective, affordable, quality medical care; and also makes, strategic long-term investments in the social determinants of health. A system that can achieve this goal must include five core elements: 1. Universal coverage; 2. an affordable defined benefit; 3. a delivery system that assumes risk and accountability for quality and outcomes; 4. a global budget indexed to a sustainable rate of growth; and 5. savings reinvested upstream in the community to address the social determinants of health.
A system that incorporates these elements can take many forms, but without all five we cannot achieve our goal of improving health care in a financially sustainable way.
The most significant obstacle to achieving this goal is the total cost of care and the structure of the delivery system that is driving it. Health care is the only economic sector that produces goods and services none of its consumers can afford. Such a system only works because the care for individuals is heavily subsidized—increasingly with public resources—either directly through public insurance programs like Medicare and Medicaid; or indirectly through the tax exclusion for employer sponsored health insurance; and the public subsidies for those purchasing insurance through the Affordable Care Act (ACA) exchanges.
For decades, the national health care debate has been focused on these subsidies—on who pays them and how much they pay—rather than on why health care costs are so much in the first place. The political paralysis around this issue is due largely to the fact that neither Republicans nor Democrats assume any change in the health care delivery model: we either pay for it or we don’t, creating a false choice between cost and access. Republicans want to spend less on health care (e.g. “repeal and replace” the ACA) while Democrats want to spend more (e.g. Medicare for All). Neither approach directly addresses the total cost of care.
The burden of rising health care costs on individuals manifests itself in a variety of ways: rising insurance premiums and deductibles, short-term insurance policies that actually cover very little, the denial of coverage based on preexisting medical conditions, surprise billing, and the high cost of prescription drugs. It is not surprising, then, that most Democratic voters blame insurance companies and drug companies for the high cost of care. Generally, consumers do not blame health care providers, the delivery system itself, or the many new health care related startups and huge private equity firms that are making a profit off the $3.5 trillion health care budget (5).
And while Democrats are right to go after short-term junk health insurance policies, huge drug price increases, and surprise health care bills, these fixes only address shortcomings with health insurance rather than the total cost of medical care. The total cost of care is the primary driver of increases in insurance premiums as well as the increase in copayments and deductibles.
Since none of the current proposals address the systemic cost of care, they cannot prevent cost shifting onto individuals. All of these short-term fixes are worth making, but they are treating symptoms of the problem, not the problem itself.
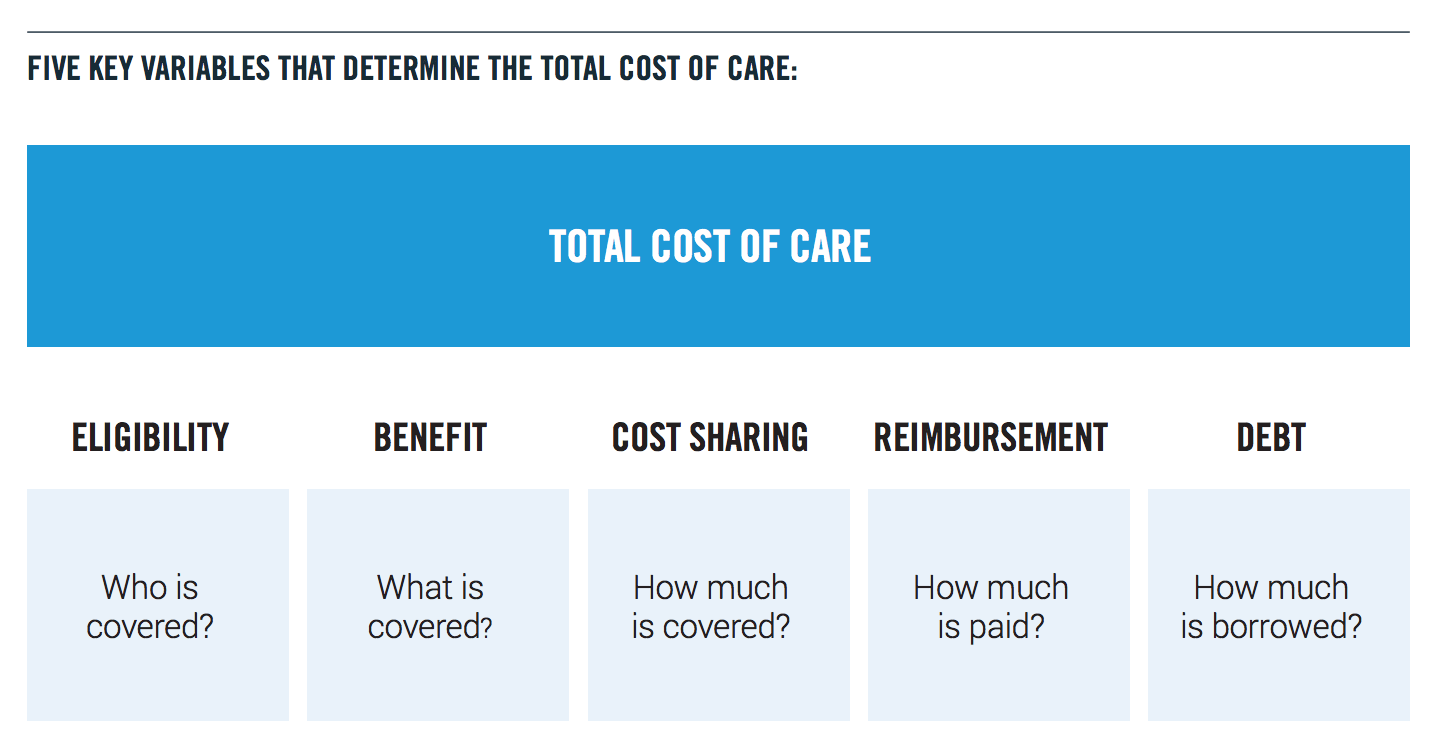
The problem is illustrated by viewing our health care system through the lens of five questions or “variables”: 1. who is covered (eligibility); 2. what is covered (benefit); 3. how much is covered (cost-sharing—e.g. premiums, copayments, deductibles); 4. how much are we paying (reimbursement); and 5. how much is borrowed (debt financing).
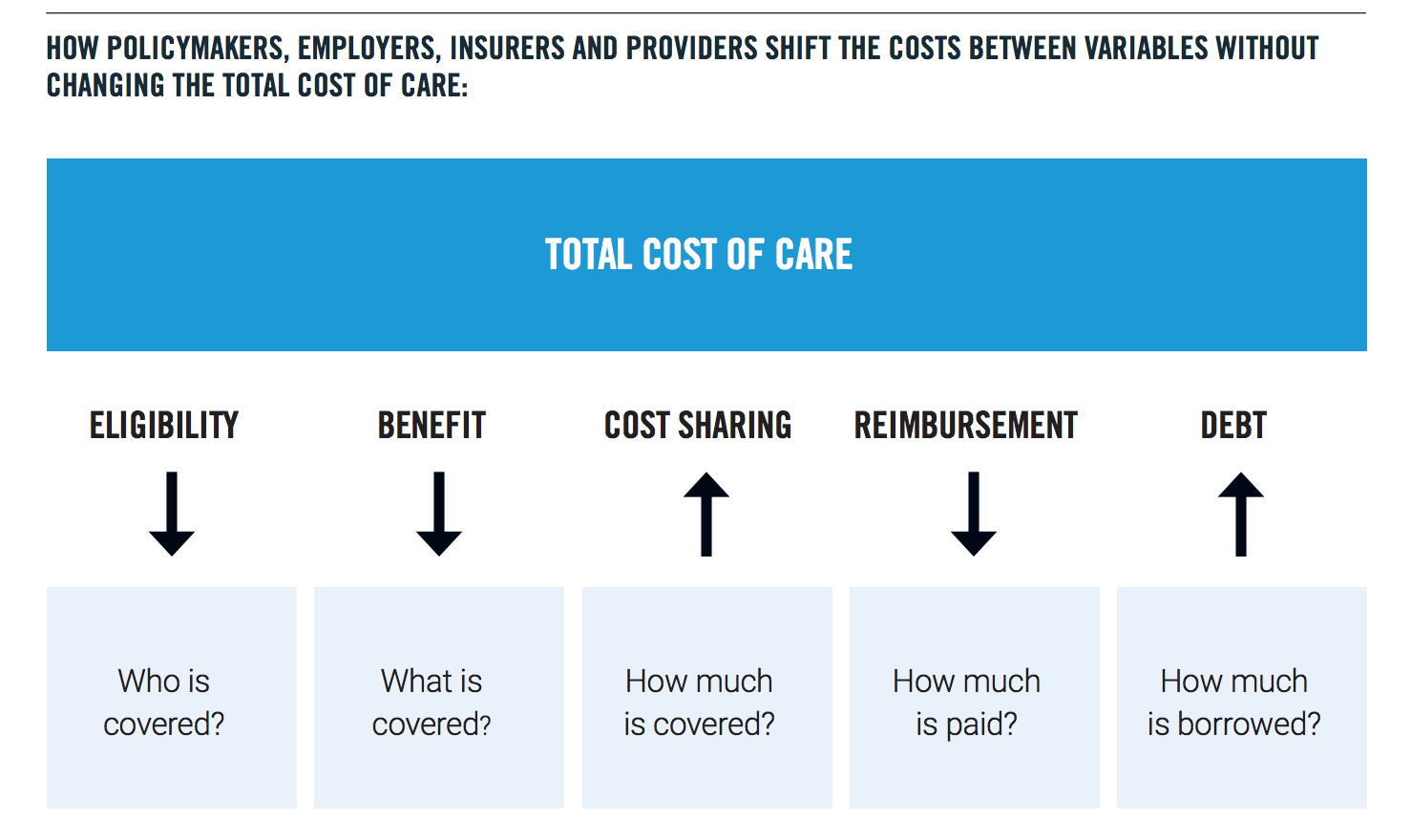
When the total cost of care exceeds the ability/ willingness of the major third-party payers (government and private sector employers) to pay for it, instead of seeking to reduce the cost of care, payers use one of five strategies to shift the cost to individuals who cannot afford it; or to future generations. These strategies include: reducing eligibility, reducing benefits and/or raising premiums, copayments and deductibles— all of which shift cost to individuals; reducing provider reimbursement which often results in efforts by providers to avoid caring for those who cannot pay; and pushing the cost of care into the national debt, shifting cost to future generations.
Cost shifting is the way we avoid directly confronting both the reality of fiscal limits and the fact that health care in the United States has simply become unaffordable for individuals, employers and the government. Cost shifting does not reduce the total cost of medical care. Furthermore, at 18 percent of our GDP, the cost of medical care, more than anything else, is undermining our ability to invest in children and families, housing, economic opportunity and the many other things that contribute to health. This is the primary reason why the U.S. has such embarrassingly poor population health statistics when compared to other industrialized nations that spend far less on medical care and far more on the social determinants (6).
The one indispensable step in moving toward a realistic and effective solution is to cap the total cost of care through a global budget indexed to a sustainable annual growth rate, while requiring providers to assume financial risk and accountability for quality and outcomes within that budget. Taking this step will fundamentally shift the debate from the subsidies to the delivery system. As long as we allow an ever-increasing share of our public resources to be spent paying whatever prices are demanded—whether for prescription drugs, hospital care or to grow profits of private equity funds—American families will continue to struggle under the burden of medical costs and this crisis will deepen.
Capping the total cost of care will allow us to expand coverage for a basic benefit package to all Americans (universal coverage); and to begin to invest upstream in the social determinants of health. The only way to expand access and to make room in the federal budget for serious investment in the social determinants of health is to reduce the total cost of care.
We already have two very successful examples of how global budgets work to bring down the total cost of care: Oregon’s Coordinated Care Organizations, which manage the state’s Medicaid program, and Medicare Advantage, that today serves more than 20 million seniors. Under these care models, providers receive a fixed amount of money for a defined population, without sacrificing quality (7). If the global budget is exceeded in any given year, the providers are at financial risk for the difference. In short, these care models begin to change the system incentives from rewarding sickness to rewarding wellness.
Extending these models more broadly across the U.S. health care system will reduce the total cost of care and free up resources to invest in the social determinants of health. It’s not necessary at this point in the 2020 election cycle to be prescriptive about how providers, insurers and other stakeholders in the current system will operate under a global budget cap indexed to a sustainable growth rate, but setting a target effective date for such a cap would fundamentally change the nature and the focus of the health care debate from where we want to go to how we are going to get there.
That is exactly what President John F. Kennedy did in 1962, when he challenged the nation to put a man on the moon. He did not give us a roadmap, he gave us a destination and, in so doing, unleashed American ingenuity and technological innovation to serve a common cause. Fifty years ago, this month, we achieved that goal. We succeeded in going to the moon because we were clear on our destination and because we imagined it; because the story preceded the accomplishment.
Surely, we can imagine linking the total cost of medical care to a sustainable growth rate within the next few years, then work backwards to create a health system that meets the objectives of both Democrats and Republicans: expanding coverage and improving health and quality; while reducing the rate of medical inflation through fiscal discipline and responsibility.
That’s the challenge. It’s not a challenge of technology—it is a challenge of political will and human compassion. And it’s not nearly as difficult as going to the moon.
Stuart M. Butler, Dayna Bowen Matthew, and Marcela Cabello, “Re-balancing Medical and Social Spending to Promote Health: Increasing State Flexibility to Improve Health Through Housing,” February 2017. https://www.brookings.edu/blog/usc-brookings-schaeffer-on-health-policy/2017/02/15/re-balancing-medical-and-social-spending-to-promote-health-increasing-state-flexibility-to-improve-health-through-housing/
Ashley Kirzinger, Cailey Muñana, Bryan Wu, and Mollyann Brodie, “Data Note: Americans’ Challenges with Health Care Costs,” The Henry J Kaiser Family Foundation, June 11, 2019, https://www.kff.org/health-costs/issue-brief/data-note-americans-challenges-health-care-costs/
Len M. Nichols and Lauren A. Taylor, “Social Determinants as Public Goods: A New Approach to Financing Key Investments in Health Communities,” Health Affaits, August 2018,https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2018.0039
Ara Ohanian, “The ROI of Addressing Social Determinants of Health,” American Journal of Managed Care, January 11, 2018, https://www.ajmc.com/contributor/ara-ohanian/2018/01/the-roi-of-addressing-social-determinants-of-health
Rabah Kamal and Cynthia Cox, “Total health expenditures have increased substantially over the past several decades,” Peterson-Kaiser Health System Tracker, December 10, 2018, https://www.healthsystemtracker.org/chart-collection/u-s-spending-healthcare-changedtime/#item-total-health-expenditures-have-increased-substantially-over-the-past-several-decades_2017
Carlyn M. Hood, Keith P. Gennuso, Geoffrey R. Swain, Bridget B. Catlin, “County Health Rankings: Relationships Between Determinant Factors and Health Outcomes,” American Journal of Preventive Medicine, 2015. https://www.countyhealthrankings.org/sites/default/files/Hood_AmJPrevMed_2015.pdf
The Institute of Medicine defines quality as “the degree to which health care services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.”
In 1901, a Colorado Springs dentist named Frederick McKay noticed many of his patients had peculiarly mottled brown teeth — but far fewer cavities than the norm. The cause, Dr. McKay determined after years of investigation, was high levels of natural fluoride in the town’s water. His discovery eventually led to the widespread fluoridation of public water systems across America and a dramatic decline in tooth decay over the past 70 years.
Numerous studies have shown the protective effects of adding fluoride to water, especially for kids, and the Centers for Disease Control and Prevention hails community water fluoridation as one of the 20th century’s top 10 public health achievements. State and local budgets have benefited too, thanks to lower public expenditures for dental care.
Here’s a question that progressives should be asking themselves: How can we encourage the development of innovative and effective treatments like Zolgensma?
Just approved by the FDA, Zolgensma is a powerful new treatment for Spinal Muscular Atrophy (SMA), which is the leading genetic cause of death in infants and toddlers. Roughly one out of every 50 adults carries one copy of the defective gene that causes SMA, and the disease affects roughly one out of every 6,000-10,000 live births.
Zolgensma—developed and marketed by AveXis, now part of Novartis—is given as a single intravenous infusion that delivers a working copy of the defective gene to motor neurons, heading off the debilitating effects of SMA. Based on the clinical trials, the positive effects of the infusion seem to persist for years.
In fact, Zolgensma is only the second gene therapy approved in the U.S. for commercial use. Since the 1970s, medical scientists have been fascinated by the idea of curing genetic diseases by modifying cell genes. However, getting to this point has been a long and winding road, punctuated by expensive setbacks and dead-ends.
Zolgensma’s success points the way to a coming future of cures and innovative treatments for debilitating diseases. That could be a triple win for progressives: Health care outcomes would improve; the long-term resource costs of healthcare to society would fall; and offering quality health care to everyone would be cheaper and easier.
But then comes the sticker shock: AveXis and Novartis are setting an initial price of $2.1 million for the one-dose treatment. For people concerned about the cost of health care, this seems like a ridiculous number.
I don’t want to get into the question of what the “right” price of the treatment should be. But based on the current medical and human cost of SMA, $2.1 million is not as big as it seems. Without a drug treatment, “best supportive care” for infantile onset SMA costs $800,000, and only yields 2.4 life-years, and less than 0.5 quality-adjusted life years (QALY). That’s according to ICER, an independent research institute.
By comparison, giving Zolgensma to pre-symptomatic infants with SMA—a usage that the FDA has approved—could give them 27 life-years and 22 QALYs, according to ICER.* How much would you pay for 25 extra years of life?
Of course, we also have to figure in how much additional medical and nursing care an infant with SMA and treated with Zolgensma will need over time. That needs to be taken into account as well.
It should be noted the initial high price of a gene therapy like Zolgensma, when introduced, may not last long. Competition from other medicines is likely to push down the price. Roche, for example, is planning to submit a new drug for treating SMA to the FDA later in 2019. In addition, AveXis and Novartis will set up 5-year payment plans for states, small insurance firms, and self-insured employers, and provide rebates if the treatment is not successful.
Many people complain that corporations take a short-term perspective and don’t take risks for the future. The truth is, for the past forty years research and development into gene therapy has been one of the best ways for the pharma and biotech sectors to lose money, since the first treatment was only approved for commercial use in 2017.
In the end, progressives who want a better-functioning and fairer healthcare system should also want as many cures and innovative and effective treatments on the market as quickly as possible. That means giving pharma and biotech companies the incentive to take the necessary risks.
*The ICER report was released before the FDA approval. But ICER analyzed what they called “Drug X,” which was the equivalent of Zolgensma given to pre-sympomatic infants.
Senator and presidential candidate Kamala Harris (D-Calif.) reintroduced her 2018 bill that seeks to address rising maternal mortality rates, particularly among black women. Harris’s Maternal CARE Act, and the accompanying House version, would authorize $150 million toward programs that seek to help medical professionals identify high-risk pregnancies and establish implicit-bias training curriculum for medical schools.
Her bill seeks to address a deeply troubling development: Severe maternal complications have more than doubled in the past 20 years and the U.S. maternal mortality rate has become the highest among high-income countries. Estimates of the maternal mortality rate span from 17.2 maternal deaths per 100,000 live births from the Centers for Disease Control (CDC) to 30.1 women per 100,000 births from the Institute for Health Metrics and Evaluation.
Last week the Trump administration announced that it would give health care workers greater leeway to refuse, on religious grounds, to provide services that enable birth control use, abortion, sterilization, or assisted suicide. Specifically, the rule bars employers from requiring their employees to participate in delivering health care services they believe their religion proscribes. Such services could include scheduling a vasectomy, prepping a room for a sex change surgery or billing for an abortion.
Democrats slammed the move, which they described as a political plum tossed to religious conservatives who form an important part of President Donald Trump’s base. If they take back the White House in 2020, it won’t take them long to reverse the rule issued by the Department of Health and Human Services (HHS) Office for Civil Rights (OCR).
The Food and Drug Administration (FDA) should be complimented for following a data-based approach to innovation and clearing the sale of heat sticks. These are new electrically heated tobacco systems that slowly heat tobacco, rather than burning it, with much fewer harmful chemical byproducts. The agency took almost two years to rigorously analyze the health impact of the innovative product, with the trade name IQOS, including the effect on the young. The goal: To give current smokers a safer alternative to health-destroying cigarettes—a “harm reduction” strategy.
A harms-reduction approach is appropriate. In 2017, the Centers for Disease Control and Prevention estimated 34.3 million adults smoke in the United States, with a public health cost of approximately $300 billion annually.
As PPI has written in the past, a harms-based regulatory approach, like the FDA took on heat sticks, is imperative to achieving advancements in both public health and economic growth. By contrast, a regulatory approach based on precaution inherently fails to maximize economic and social benefits.
Indeed, we also applaud the FDA for paying attention to social benefits and costs. For example, with recent concern over rising youth smoking in the U.S., the FDA rightfully placed restrictions on how heat sticks are marketed to youth. The restrictions limit how heat sticks are marketed via websites and on social media by requiring advertising to be targeted to adults. Heat stick manufacturers must also notify the FDA about how they plan to restrict youth access and limit youth exposure to the products’ marketing.
Too many Americans lack access to dental care, especially in underserved areas. Forty-four percent of people below the federal poverty level have untreated dental decay compared to just 9.5 percent of those above 400 percent of the federal poverty level.
The consequences of untreated decay and periodontal disease – slowly destructive gum infections – include increased risk of cancers, cardiovascular diseases, Alzheimer’s disease, and pre-term delivery among pregnant women. Furthermore, poor oral health can change how people eat, work and live their lives. Oral health reflects people’s social determinants of health and can reinforce poverty.
Last week PPI returned to Des Moines for a second “Conversation with Iowans,” this time about progressive alternatives to nationalized health care. The ideas forum featured former Colorado Gov. and presidential aspirant John Hickenlooper, Theresa Greenfield, a Des Moines business owner, PPI President Will Marshall and yours truly.
A strong turnout and often impassioned debate underscored that health care — the fear of losing it or not being able to afford it — is still a burning issue for Americans, just as it was during last year’s midterm election. Many participants told gut wrenching personal stories about their maddening interactions with our complex and costly health delivery system. One woman, for example, relayed how her Type 1 diabetes diagnosis had led to multiple hospital stays, medical debt, and anxiety every month over covering her insulin costs.
When it comes to health care, Americans could not face a clearer choice. Progressives believe all Americans should have access to affordable, high-quality health coverage. Republicans want to kill the Affordable Care Act – thereby depriving an additional 17 million Americans of insurance – and have no credible plan to replace it. Too often, however, the health care debate focuses on how to pay for health insurance rather than how to deliver better health care.
PPI believes producing better outcomes at lower prices must be the first principle of health care reform, and share a vision for health care reform in Des Moines, Iowa on Friday, April 12th.
He has broken every one of those promises over the last two years. What’s more, the White House campaign to sabotage the Affordable Care Act (ACA) sparked a voter backlash that cost Republicans dearly in last year’s midterm election.
The president apparently has learned nothing from that rebuff. Having failed to pass legislation to kill the ACA, the administration is now turning to judicial activism and the courts. The Department of Justice (DOJ) announced yesterday that it is endorsing a Texas court ruling striking down the entire ACA.