We are seeing two important, and in some ways, potentially contradictory trends in manufacturing these days. On the one hand, there are signs of a transformation and rebirth in domestic manufacturing. Technological innovations such as 3D printing and robotics are lowering the cost of manufacturing at home, while global trade tensions are leading companies to shorten their supply chains (1). This raises the possibility of a new round of job creation in local domestic manufacturing.
At the same time, states are increasingly moving to tighten their oversight and regulation of chemicals, especially those in consumer products. For example, the state of Washington just adopted “The Pollution Prevention for Our Future Act,” billed as the strongest such measure in the country. The New York State legislature has recently passed legislation regulating chemicals in children’s products. In the same vein, Vermont’s legislature just passed a bill strengthening and broadening existing rules for disclosure of chemicals in children’s products.
Increased attention to safety is not a bad thing. We can have innovation and safety in manufacturing, while still encouraging growth and jobs.
But let’s be honest: state governments do not have the budgetary resources to assess the risk of hundreds of chemicals. As a result, state regulators and legislatures are reaching out globally and relying on lists of chemicals assembled by highly trusted authorities around the world, in addition to any information from the U.S. federal government. For example, in the U.S., states such as Maine, Minnesota, and California, among others, have relied on the E.U.’s conclusions about certain chemicals when crafting their Chemicals of Concern lists, which prioritize chemicals for further reporting, study, and/or possible regulation. Canada and Australia also have agencies that are well respected in assessing potential risks from chemicals.
In drawing on other parts of the world, states must be aware that these authorities can analyze the same data and come to different –and even conflicting – conclusions depending on the principles their regulatory regime is founded on. The E.U., for example, tends to take a “hazard-based” approach founded on the precautionary principle, which holds that “when an activity raises threats of harm to human health or the environment, precautionary measures should be taken even if some cause and effect relationships are not fully established scientifically” (2). The precautionary principle generally leads to more skepticism about innovative materials and technologies. As a result, the E.U. identifies chemicals as “Substances of Very High Concern” (SVHC) purely on the basis of their hazardous properties, such as being very persistent and very bioaccumulative (vPvB).
By contrast, Canada, Australia, and the U.S. have tended more towards a risk-based approach to regulation. A risk-based approach focuses not only on the theoretical potential for harm, but actual harm. If no actual harms can be measured, the action or product is allowed, and no regulatory action is taken.
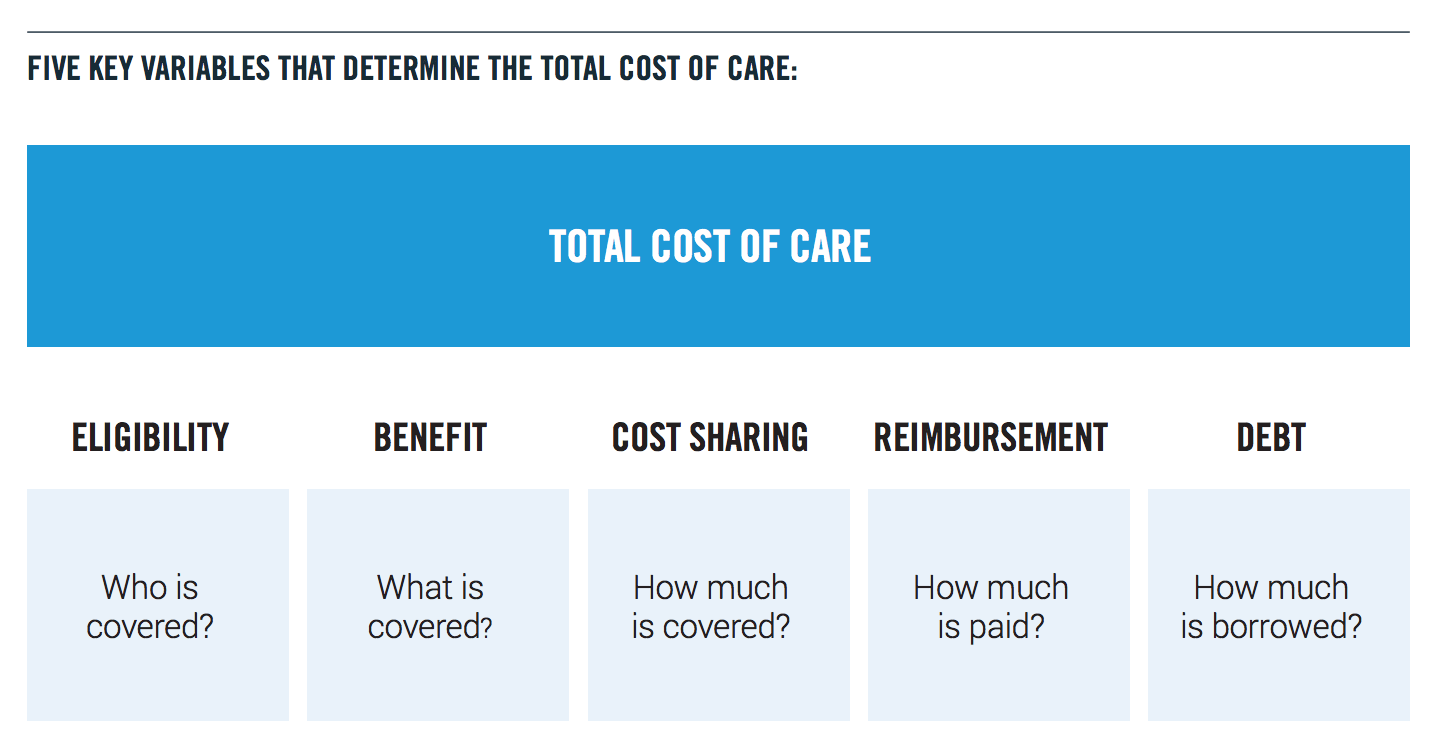
Thus, a state’s choice of reference for regulating chemicals is not purely a technical matter. It is important for states to realize the different approaches to chemicals regulation at hand, and the economic consequences the approach they opt for could have. Chemicals are a sizeable industry in the U.S. economy, with total sales of $493.4 billion in 2017, according to a 2018 industry report (3).
More importantly, the approaches states take to chemicals regulation has powerful implications for jobs and economic growth in the future. The next wave of tech-based innovation will come in such physical industries as manufacturing and will be driven in part by new materials and new processes. Excessively stringent regulatory regimes or blacklisting certain chemicals will unnecessarily squelch innovations that could establish a new digital manufacturing sector that creates local jobs.
This paper will first describe how states use their limited resources to focus their chemical regulation. We will then contrast the precautionary principle with the risk-based approach, using siloxanes as an example. Specifically, as the Progressive Policy Institute wrote in a previous paper, siloxanes octamethylcyclotetrasiloxane (also known as “D4”), decamethylcyclopentasiloxane (also known as “D5”), and dodecamethylcyclohexasiloxane (also known as “D6”) have been assessed by the E.U., Canada, and Australia for their impact on human health and the environment (4). In the U.S., states such as Maine, Minnesota, and California, among others, have relied on the E.U.’s conclusions when crafting their own Chemicals of Concern lists. Contrastingly, Canada has chosen not to restrict the use of siloxanes, and other states, including Washington State and Oregon, have removed siloxanes from their lists due to the lack of evidence of real-world harm.
Finally, we will examine the economic implications of the differing regulatory approaches.
The Limited Resources of States
State governments simply do not have the budgetary resources to test chemicals themselves. As a result, they rely on federal or international governments to conduct the scientific research that forms the rationale for much of their health and environmental legislation and regulation. After all, why would states duplicate research that those governments have already done?
One example of this is in state Chemicals of Concern lists, where some U.S. states have imported lists of chemicals from trusted sources such as the U.S. federal government, the E.U., and Canada. For instance, Maine includes chemicals on its Chemicals of Concern list that have been listed by another authoritative governmental entity as being harmful to human health or the environment (5). These entities include the U.S. Department of Health and Human Services (HHS), Food and Drug Administration, Centers for Disease Control and Prevention, EPA, and the European Chemicals Agency, among others.
Similarly, Minnesota’s Chemicals of High Concern list was sourced by “reviewing the hazard characteristics of chemicals studied by other state, national and international agencies” (6). These agencies include Maine’s Chemicals of Concern List, the U.S. HHS, the U.S. EPA, and the European Parliament’s Authorization List under the REACH regulation (7).
California imports chemicals for its Candidate Chemicals List based on their inclusion on other authoritative lists, such as the E.U.’s substance of very high concern (SVHC) list, Canada’s Domestic Substances List, and the U.S. EPA’s Integrated Risk Information System, among others (8).
Vermont’s existing Chemicals of High Concern to Children list requires the Vermont Health Commissioner to review the list every two years to determine if additional chemicals should be added, considering “designations made by other states, the federal government, other countries, or other governmental agencies,” including the E.U.’s SVHC list (9). The state’s new legislation would make it even easier to add chemicals to the list.
Washington State uses “authoritative sources that identify chemical toxicity…and evidence of potential for exposure” to craft its Chemicals of Very High Concern to Children list.10 The authoritative sources include the U.S. EPA’s Integrated Risk Information System, the E.U.’s SVHC list, and the International Agency for Research on Cancer, among others.
And Oregon’s Health Authority uses “guidance developed by the State of Washington and other federal, state and nongovernmental organizations” to create its Chemicals of Concern for Children’s Health list (11).
The Risk-Based Approach vs. The Precautionary Principle
However, the importation of chemicals lists from different authoritative sources can lead to different outcomes for states, depending on the principles the regulatory regime of the authoritative source is founded on. Regulation in the E.U. tends to be rooted in a hazard-based approach that is founded on the precautionary principle, or the belief that “when an activity raises threats of harm to human health or the environment, precautionary measures should be taken even if some cause and effect relationships are not fully established scientifically” (12). This hazard-based approach is consistent with the E.U.’s skeptical approach to innovation in general.
Conversely, Canada and Australia tend to opt for a risk-based approach where all available scientific evidence is evaluated. A risk-based approach requires harms to be identified and measured. Harms can include impact to human health, the environment, or to the economy. If no harms can be identified, the product or action is permitted to continue, and no regulatory action is taken.
Take for example siloxanes, which the E.U. added to its SVHC list based on characterizing them as “persistent, bioaccumulative and toxic” (PBT) or “very persistent and very bioaccumulative:” (vPvB). Some states have drawn on the E.U.’s assessment when creating their own chemicals of concern lists (13). California includes siloxanes D4, D5, and D6 on its Candidate Chemicals List, based on the siloxanes’ presence on the E.U.’s SVHC list (14,15,16,17).
Maine uses the presence of a chemical on its Chemicals of Concern (COC) list that meets additional toxicity and exposure criteria for inclusion on its Chemicals of High Concern (CHC) list (18). As a result, D4 has been included on the state’s most recent 2015 CHC list based on the E.U.’s toxicity assessment (19). Similarly, D5 has remained on Maine’s Chemicals of Concern list based on E.U. findings. Contrastingly, D6 was removed from Maine’s COC list because of the lack of assessments by authoritative institutions (20).
In Minnesota, D4 was included on its most recent 2016 Chemicals of High Concern list based on appearing on Maine’s 2015 Chemicals of High Concern list.21 And D4 is listed on Vermont’s list of Chemicals of High Concern to Children. Like Maine, the inclusion is based on its assessment by the E.U (22).
Contrastingly, Canadian regulators initially found D4 and D5 to be harmful to the environment and, as such, both substances could possibly have been subject to regulatory measures to lessen the substances’ impact on the environment (23, 24). However, an independent review board of experts analyzed a wealth of available data, including studies that showed the real-world behavior of D5, and concluded “there is no evidence to demonstrate that Siloxane D5 is toxic to any organism tested up to the limit of solubility in any environmental matrix” (25).
In terms of D4, a government-funded environmental monitoring study, which measured real-world concentrations of D4, D5, and D6 in the environment, found very low levels of D4 in Canadian surface waters (26). Rather than restricting or banning the substance’s use in consumer or industrial products, the Canadian government required certain facilities that use D4 to implement pollution prevention plans (27).
Australian regulators came to similar conclusions when they determined that product restrictions or bans on D4, D5, and D6 were not necessary because evidence demonstrated that “[t]he direct risks to aquatic life from exposure to these chemicals at expected surface water concentrations are not likely to be significant” (28).
Similarly, some states have revised their Chemicals of Concerns lists, based on additional study by other authoritative bodies. Washington State initially included D4 on its Chemicals of High Concern to Children (CHCC) list based on its inclusion on the E.U.’s priority list for Category 1 Endocrine Disruptors. But following a detailed review of the available evidence, including a study funded by the U.S. National Institutes of Health, the Washington State Department of
Ecology concluded (30):
“D4 is present on the European Commission (EC) Category 1 list, based on a single study, showing an increase in uterine weight (McKim et al, 2007). However, a more recent study shows no effect on uterine weight by D4 (Lee et al, 2015). These mixed results, along with biomarker and in vitro data for D4 (He et al, 2003; Quinn et al, 2007; Lee et al, 2015) are not sufficient for CHCC listing…D4 is not listed by any of the other CSPA authoritative sources. D4 does not meet the CHCC listing criteria” (31).
And, because Oregon’s list is primarily sourced from Washington State’s list, Oregon also removed D4 from its High Priority Chemicals of Concern for Children’s Health list (32).
The authoritative sources that states use when crafting their own chemicals of concern lists has resulted in binary outcomes. A regulatory approach founded on precaution (such as California, Maine, and Minnesota have imported) inherently prohibits innovation. States like California, Maine, Minnesota, and Vermont, who have crafted their lists from inclusion based on the E.U.’s Category 1 Endocrine Disruptor program or SVHC lists, have taken a step toward identifying the chemicals as priority chemicals, putting siloxanes or products containing them on the road to regulation and potential ban.
Moreover, manufacturers do not want to be associated with any listed chemicals, so they stay away from them even if chemicals have not been officially banned.
For example, in Vermont, manufacturers of children’s products using chemicals of high concern to children are required to report to the state when the chemicals are used in a significant amount, and the law allows the Health Commissioner to consider banning the sale of products including the chemical (33).
In California, inclusion on the Candidate Chemicals List is an action toward listing products as a “priority product,” which would require businesses manufacturing the siloxanes to notify the California Department of Toxic Substances Control (DTSC) if their product is listed. The designation would also allow the DTSC to take other regulatory actions such as limiting the siloxanes’ use or requiring companies to replace it with an alternative (34).
Meanwhile, Washington State removed siloxanes from its list after taking a “weight of evidence” approach and analyzing all available evidence for real-world harm to human health or the environment. This approach permits advancements in innovation and growth to be realized unless evidence of real-world harm can be found.
Economic Implications of Chemical Regulation
The regulatory approach states take to silicones regulation has implications for jobs and economic growth not just today, but also in the future. Indeed, silicones are an input in many industries including construction, electronics, health care, household products, renewable energy technologies and personal care products, to name a few. A 2016 industry report estimated total sales of silicones products in the Americas to be $3.1 billion in 2013, with the highest consuming industries being industrial processes, construction, and personal care and consumer products (35). Restricting these materials will raise prices for both manufacturers and the industries that utilize silicones.
What’s more, the rebirth of manufacturing jobs in the U.S. will rely on new technologies such as 3D printing, which themselves rest on the creation of new and reformulated materials. As the Progressive Policy Institute (PPI) pointed out in a 2018 paper, “the range of materials that can be 3D printed is constantly expanding. Desktop Metal is expected to come out with a metal 3D printing system for mass production in 2019. HP plans to launch a line of 3D printers that produce metal objects, an expansion from the company’s existing 3D printers that produce plastic-based products” (36).
Take German chemical company Wacker Chemie for example, who in 2016 discovered how to 3D print silicones, a process that requires heating and binding a material that is naturally heat-resistant to manufacture goods (37). This innovation will open up new markets for manufacturers in critical areas of application such as medicine, where silicone is considered to be bio-compatible and durable. Silicone 3D printing also enables manufacturers to cut production costs, become more efficient, and enable new business models upon which new U.S. manufacturing jobs would be based.
New and reformulated materials will also be needed to revitalize the construction sector, where productivity growth has lagged and the cost of construction has doubled since 2000, as PPI wrote in a 2017 report (38). One of the contributors to rising prices in the sector was the cost of materials, as certain asphalt products, paving mixtures, and steel products are nearly twice as expensive today as they were in 2000. Innovation in materials would help revitalize productivity and economic growth in the sector.
If states move to blacklist or even prohibit silicones based on the E.U.’s lists rooted in the precautionary principle rather than on real-world scientific evidence, that is not a good sign for the regulatory attitude toward new materials with less of a track record.
Indeed, the broader danger is that a strict precautionary approach to chemical listing
and regulation, as would be implied by tighter regulation of silicones, would have negative implications for the rebirth of manufacturing jobs in the U.S. After all, under states importing lists from the E.U., the companies that manufacture and use new materials would have to be able to conclusively prove their lack of impact on human health and the environment in order to continue using them.
Conclusion
State governments do not have the budgetary resources to test or evaluate chemicals themselves. As a result, they rely on national and international governments to conduct the research and assessments that form the basis of health and environmental regulation. But, depending on the underlying principles of the authoritative source’s regulatory regime, states could end up with different conclusions.
Siloxanes provide a prime example of these differences in approach. The E.U. has designated them as substances of very high concern and have moved to restrict the use of silicones in certain products, based on being “very persistent and very bioaccumulative.” By contrast, Canada and Australia have taken a weight of evidence approach, analyzing all the available evidence and requiring real-world harm to the environment or human health before taking regulatory action.
The result has led to different outcomes. While states relying on the E.U.’s SVHC list and related criteria have put D4, D5, and D6 on a path to regulation, states that have taken a weight-of-evidence approach similar to Canada and Australia have removed silicones from their Chemicals of Concern list and allowed the silicones unrestricted in the marketplace. If states are to develop Chemicals of Concern lists at all, state policymakers should consider basing those lists only on authorities that evaluate chemicals utilizing a risk-based approach. This would decrease instances where substances that pose little or no risk, like siloxanes, are blacklisted unnecessarily.
These divergent outcomes have implications for jobs and economic growth today and in the future. Silicones are a multi-billion-dollar industry in the Americas and an input in many goods and services, including industrial processes, construction, healthcare, and personal care and consumer products.
What’s more, the rebirth of manufacturing jobs in the U.S. will rely on new technologies such as 3D printing, which themselves require the creation of new and reformulated materials. Silicones will play a critical role in realizing new materials that will revitalize other industries such as manufacturing and construction, where productivity and job growth has lagged for years.
Indeed, precautionary regulation of silicones by states, rather than risk-based, does not indicate regulators are prioritizing innovation. Rather, it signals negative implications for the revitalization of historically important industries to the U.S. economy.
REFERENCES
1) Michael Mandel, “The Trade War Spreads to Mexico, And The Window Opens Wider for Digital Manufacturing,” https://www.forbes.com/sites/michaelmandel1/2019/05/31/the-trade-war-spreads-to-mexico-and-the-window-opens-wider-for-digital-manufacturing/#27a94a784589
2) “Wingspread Conference on the Precautionary Principle,” Science and Environmental Health Network, January 26, 1998.
3) “2018 Elements of the Business of Chemistry,” American Chemistry Council. https://www.americanchemistry.com/2018-Elements-of-the-Business-of-Chemistry.pdf
4) Elliott Long and Michael Mandel, “Science-based Regulation and Innovation: The Silicone Example,” Progressive Policy Institute, May 2018. https://www.progressivepolicy.org/wp-content/uploads/2018/05/PPI_Silicones-Paper-2018.pdf
5) “Chemicals of High Concern Triennial Update Documentation,” Maine Center for Disease Control and Prevention, July 21, 2015.
6) “Toxic Free Kids Act: Chemicals of High Concern – Frequently Asked Questions,” Minnesota Department of Health, July 2010. https://www.health.state.mn.us/communities/environment/childenvhealth/tfka/faq.html#how
7) “Minnesota Chemicals of High Concern List Methodology,” Minnesota Department of Health, July 1, 2010. https://www.health.state.mn.us/communities/environment/childenvhealth/docs/chlist/methodology.pdf
8) “§ 69502.2. Candidate Chemicals Identification,” California Department of Toxic Substances Control. https://dtsc.ca.gov/wp-content/uploads/sites/31/2018/10/69502-2-Candidate-Chemicals-Identification.pdf
9) “No. 188. An act relating to the regulation of toxic substances, §1773.” Vermont Department of Health. https://www.healthvermont.gov/sites/default/files/documents/2016/11/Env_CDP_ACT188_0.pdf
10) “Children’s Safe Products Reporting Rule Rationale for Reporting List of Chemicals of High Concern to Children 2011-2017,” State of Washington Department of Ecology, November 2018. https://fortress.wa.gov/ecy/publications/documents/1804025.pdf
11) “S.B. 478, the Toxic Free Kids Act,” 78th Oregon Legislative Assembly – 2015 Regular Session. https://olis.leg.state.or.us/liz/2015R1/Downloads/MeasureDocument/SB478
12) “Wingspread Conference on the Precautionary Principle,” Science and Environmental Health Network, January 26, 1998.
13) Regulation (Ec) No 1907/2006 Of The European Parliament And Of The Council
14) “Candidate Chemicals List,” California Department of Toxic Substances Control. https://dtsc.ca.gov/scp/authoritative-lists/
15) “Octamethylcyclotetrasiloxane (D4),” California Department of Toxic Substances Control. https://calsafer.dtsc.ca.gov/cms/candidate-chemical/?rid=21382&from=search
16) “Decamethylcyclopentasiloxane (D5),” California Department of Toxic Substances Control. https://calsafer.dtsc.ca.gov/cms/candidate-chemical/?rid=21353&from=search
17) “Dodecamethylcyclohexasiloxane (D6),” California Department of Toxic Substances Control. https://calsafer.dtsc.ca.gov/cms/candidate-chemical/?rid=21352&from=search
18) “Chemicals of High Concern Triennial Update Documentation,” Maine Center for Disease Control and Prevention, July 21, 2015.
19) “Chemicals of High Concern 2015 Triennial Update,” Maine Center for Disease Control and Prevention, July 21, 2015.
20) Kyle Brown, “Silicone regulations evolve globally,” Rubber & Plastic News, April 30, 2018. https://www.rubbernews.com/article/20180430/NEWS/180509999/silicone-regulations-evolve-globally
21) “The 2016 Minnesota Chemicals of High Concern List,” Minnesota Department of Health. https://www.health.state.mn.us/communities/environment/childenvhealth/docs/chlist/mdhchc2016.pdf
22) “Octamethylcyclotetrasiloxane (D4),” Vermont Department of Health. https://www.healthvermont.gov/sites/default/files/documents/pdf/ENV_CDP_556_67_2_Octamethylcyclotetrasiloxane.pdf
23) “Siloxane D4 (Cyclotetrasiloxane, octamethyl-),” Government of Canada. https://www.canada.ca/en/health-canada/services/chemical-substances/challenge/batch-2/cyclotetrasiloxane-octamethyl.html
24) “Siloxane D5 (Cyclopentasiloxane, decamethyl-),” Government of Canada. https://www.canada.ca/en/health-canada/services/chemical-substances/challenge/batch-2/cyclopentasiloxane-decamethyl.html
25) “Report of the Board of Review for Decamethylcyclopentasiloxane (Siloxane D5),” Environment and Climate Change Canada. https://www.ec.gc.ca/lcpe-cepa/default.asp?lang=En&n=515887B7-1&offset=7&toc=show
26) De-Gao Wang, Helena Steer, Tara Tait, Zackery Williams, Grazina Pacepavicius, Teresa Young, Timothy Ng, Shirley Anne Smyth, Laura Kinsman, and Mehran Alaee. “Concentrations of cyclic volatile methylsiloxanes in biosolid amended soil, influent, effluent, receiving water, and sediment of wastewater treatment plants in Canada,” Chemosphere, November 2012.
27) “Siloxane D4 in industrial effluents: pollution prevention planning notice,” Environment and Climate Change Canada. https://www.canada.ca/en/environment-climate-change/services/pollution-prevention/planning-notices/performance-results/siloxane-d4-industrial-effluents-overview.html
28) https://www.nicnas.gov.au/chemical-information/imap-assessments/imap-assessments/tier-ii-environment-assessments/cvms
29) “Children’s Safe Products Reporting Rule: Rationale for Reporting List of Chemicals of High Concern to Children 2011-2017,” State of Washington Department of Ecology, November 2018. https://fortress.wa.gov/ecy/publications/documents/1804025.pdf
30) Lee D, Ahn C, An BS, Jeung EB. (2015) Induction of the estrogenic marker calbindn-d9k by octamethylcyclotetrasiloxane. Int J Environ Res Public Health 12:14610-25. https://www.ncbi.nlm.nih.gov/pubmed/14575643
31) “Concise Explanatory Statement, Chapter 173-334 WAC, Children’s Safe Products Reporting Rule: Summary of rulemaking and response to comments,” State of Washington Department of Ecology, September 2017. https://fortress.wa.gov/ecy/publications/documents/1704034.pdf
32) “U.S. – Oregon Amends Toxic-Free Kids Rule,” Intertek, October 02, 2018. https://www.intertek.com/consumer/insight-bulletins/oregon-amends-toxic-free-kids-rule/
33) “Safer Chemicals in Children’s Products Rules: Regulation of Chemical Use in Children’s Products: Chapter 880,” Maine Department of Environmental Protection. https://www.maine.gov/dep/safechem/rules.html
34) “How Do the Priority Products Affect Me?,” California Department of Toxic Substances Control. https://dtsc.ca.gov/scp/how-do-the-priority-products-affect-me/
35) “Socio-economic evaluation of the global silicones industry: regional summary – the Americas,” Global Silicones Council, March 2016. https://sehsc.americanchemistry.com/Socio-Economic-Evaluation-of-the-Global-Silicones-Industry-The-Americas.pdf
36) Michael Mandel, “The Rise of the Internet of Goods: A New Perspective on the Digital Future for Manufacturers,” MAPI Foundation and Progressive Policy Institute, August 7, 2018. https://www.progressivepolicy.org/wp-content/uploads/2018/08/Internetofgoods-reportPPI-2018 .pdf
37) “Silicone 3D Printer – All You Need to Know in 2019,” All3DP.com. https://all3dp.com/2/silicone-3d-printer-all-you-need-to-know/
38) Elliott Long, “Soaring Construction Costs Threaten Infrastructure Push,” Progressive Policy Institute, October 2017. https://www.progressivepolicy.org/wp-content/uploads/2017/10/PPI_Construction_2017.pdf