INTRODUCTION
Democrats have made extending a pandemic-era expansion of the Affordable Care Act’s (ACA) premium tax credit (PTC) their central demand in this year’s government funding negotiations, going so far as to threaten a government shutdown next week if Republicans do not attach it to a short-term funding bill. The pandemic PTC served an important purpose in the midst of the COVID-19 pandemic, helping reduce the cost of health insurance for households that did not have coverage through their employer or another government program at a time when workers were at heightened risk of losing their jobs or experiencing a medical emergency. It also corrected some long-standing problems with the PTC’s original structure, such as a “benefit cliff” that discouraged earnings by cutting benefits off altogether for households that made even one dollar more than the income eligibility limit.
Allowing the expansion to expire immediately in its entirety, as most Republicans propose to do, would be deeply damaging: the Congressional Budget Office (CBO) estimates that more than 4 million Americans could lose their health insurance when the pandemic PTC expires, while the Kaiser Family Foundation (KFF) estimates that out-of-pocket premium payments for enrollees on the individual insurance exchange marketplaces would rise by more than 75%.
But reflexively continuing the policy in its current form, whether through repeated temporary extensions or outright making it permanent, would also be unwise. The pandemic PTC provides substantial subsidies for households higher up the income ladder that go far beyond the program’s original intent. The extension is expensive, costing more than $20 billion per year — a cost Democrats never proposed to sustainably pay for, despite the national debt already being at historic heights. The tax subsidies it provides for a small slice of the population are significantly more costly than the tax subsidies from which most Americans benefit through employer-sponsored insurance. And perhaps worst of all, the pandemic PTC pumps more money into a broken and costly health-care system while doing nothing to tackle the true drivers of high prices.
PPI proposes a pragmatic path forward between these two extreme positions. Our proposed framework would gradually transition into a new PTC structure somewhere between the original PTC and the pandemic PTC — one that eliminates the benefit cliff without showering unnecessary tax subsidies on high-income households. Moreover, we propose to pair this policy with other changes that more than offset its cost to the federal budget while reducing the price of health care for taxpayers and patients alike.
THE PANDEMIC PTC MAKES THE ACA MORE REGRESSIVE AND EXPENSIVE
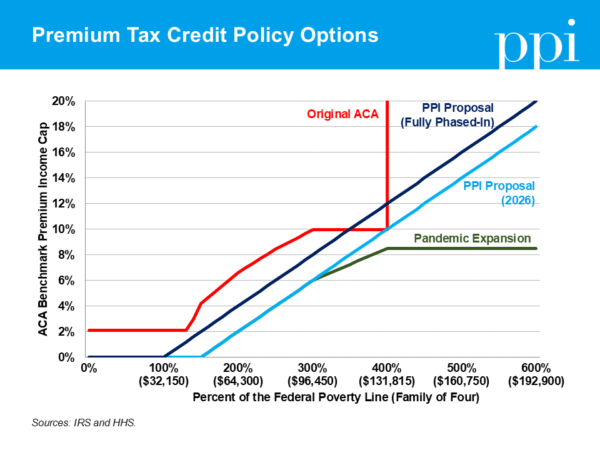
The original PTC was created by the ACA in 2014 to ensure that Americans who did not receive health insurance from the government or their employer could still afford quality health insurance. The ACA established thresholds for affordable health insurance based on income: for an American at the Federal Poverty Level (FPL), that affordability threshold could be just 2% of their income, while a middle-income American could be asked to pay up to 10%. If the cost of a benchmark plan exceeded this affordability threshold, enrollees with household incomes below 400% of FPL would receive a premium tax credit to make up the difference, which they could use to purchase any insurance plan on the ACA’s individual marketplace exchanges.
Even before the pandemic, the PTC had been unintentionally expanded through the practice of “silver-loading.” Insurers raised the cost of their middle-tier “silver” plans, which serve as the benchmark plans for PTC calculations, even though costs for both cheaper “bronze” and premium-tier “gold” plans on the exchanges remained unchanged. This practice increased PTC payments across the board, meaning households shopping on the exchanges could purchase a higher-quality plan using a smaller share of their income than the affordability threshold dictated.
The American Rescue Plan Act (ARP) passed during the COVID-19 pandemic then made the PTC significantly more costly — and less progressive — by lowering the affordability threshold across the board and making all households eligible for the PTC regardless of income for 2021 and 2022. The Inflation Reduction Act (IRA) extended this pandemic PTC expansion for an additional three years, but the policy is set to expire at the end of this year.
On the positive side, the pandemic PTC expansion fixed one of the greatest problems with the original PTC, whereby recipients could lose several hundred dollars of tax credits if they earned just one dollar over the 400% of FPL eligibility limit. It also made health insurance significantly more affordable during a once-in-a-century pandemic in which many people faced the sudden loss of income and insurance, along with higher medical risk.
But the pandemic PTC was never designed as a thoughtful long-term policy. Median-earning households are now expected to pay only two-thirds what the original ACA intended them to pay for a benchmark plan, and households with income below 150% of FPL are expected to pay no premium whatsoever. Even worse, the combination of a low benchmark premium cap with no eligibility limitation results in very high-income households receiving subsidies that were never intended for them when the ACA became law. In New York City, for example, couples with no children earning 1,000% of FPL — more than double the original PTC’s eligibility limit — are currently eligible for a PTC of more than $3,000 per year.
Those costs all add up: today, the average annual subsidy for the 7% of Americans who are covered by ACA exchange plans is $6,600 per person. That’s more than three times the tax subsidy that benefits people with employer-sponsored insurance, who make up more than half the population. These costs were worth the benefits during a global public health emergency, but they make little sense to continue as permanent policy — especially since supporters never determined a way to pay for them at a time when the government is running $2 trillion annual budget deficits.
Yet Democrats have rallied around legislation to extend the pandemic PTC permanently, which would cost approximately $380 billion over the next 10 years. At a minimum, they — and even a few Republicans — have argued in favor of extending the expiring subsidies for one year at a cost of $23 billion. But nobody has offered a coherent rationale for why it would make more sense to phase down subsidies next year than this year, especially considering that it is a midterm election year. A one-year extension with no adjustments or strings attached now simply sets the stage for more extensions in the future as a backdoor attempt to make the policy permanent.
Democrats must move beyond the desire they’ve shown in recent years to reflexively extend expiring pandemic-era policies that were never designed as long-term solutions. There is a better approach that prevents sharp premium hikes for families and eases into a more sustainable long-term policy while permanently fixing the benefit cliff and leaving health care more affordable for families than it was before the ARP.
PPI proposes to gradually move towards a reworked PTC structure that is more progressive and fiscally sustainable than the pandemic PTC, yet more fair than the original ACA. In 2026, households with incomes under 300% of FPL should be eligible for the same enhanced subsidies created by ARP. But the affordability threshold should continue to rise for higher earners rather than being capped at 8.5%. This will result in higher-income households gradually receiving lower subsidies as their income rises, and will fully phase out subsidies at lower income levels than they do today.
Then, over the next two years, the beginning of the phase-in for higher affordability thresholds would gradually move from 150% of FPL in 2026 to 100% of FPL in 2028. This compromise offers free health insurance for families in poverty while requiring modest contributions from middle-income households that can afford it and tapers off support for high-income households that don’t need it. Policymakers can choose at this point whether they would make the new subsidy structure permanent or let voters decide its future in the 2028 elections. Based on modeling from the Committee for a Responsible Federal Budget, we estimate this proposal will cost roughly $200 billion over 10 years if made permanent, relative to allowing the pandemic PTC to expire at the end of this year.
CONGRESS MUST TACKLE THE REAL DRIVERS OF HEALTH COSTS
The other flaw with simply extending the pandemic PTC is that it doesn’t address the real problem of rising health-care costs, which have dramatically increased over time relative to the size of the economy. In 1963, health-care costs represented 5% of Gross Domestic Product (GDP). In 2025, they are projected to reach 18.5% of GDP. Today, the average cost of health care in the United States is estimated to be more than $16,500 per person, which historically has been nearly twice as much as the average cost of health care per person in other wealthy countries.
Expanding subsidies for a small slice of the population without tackling the drivers of high health-care costs will only fuel further price increases. When government assistance covers a larger share of premiums, insurers and providers face less pressure to control spending, allowing them to charge more knowing that taxpayers will pick up the bill. Prices climb in response, and costs to families and the federal budget escalate. It would therefore be both good policy and good politics to ensure that Americans who benefit from the PTC keep their health insurance while also confronting the structural reasons behind rising health-care costs.
Fortunately, there are smart reforms that policymakers can and should pair with any PTC expansion to both offset their cost to taxpayers and tackle the root causes of rising health-care costs. One place lawmakers should start is Medicare Advantage, which allows seniors to receive their Medicare benefits from private insurers rather than the federal government. While this program was originally intended to save money, it now costs taxpayers tens of billions of dollars per year because of loopholes that allow insurance companies to inflate their government reimbursements without increasing the quality of their care.
Through Medicare Advantage, insurance companies are paid based on the number of seniors they cover, plus an adjustment for enrollees’ “risk scores,” based on their health history. This mechanism was designed to compensate insurers for covering sicker, more expensive seniors. But insurers have manipulated the system through a practice called upcoding, which entails inflating patients’ risk scores with questionable diagnoses in order to make them appear sicker than they really are. Insurers use a variety of tactics to increase risk scores, including pushing patients to complete health risk assessments with company-employed providers and combing through patients’ medical records in chart reviews to look for diagnoses that doctors never reported.
In order to curb these overpayments, Congress should adopt key provisions from the bipartisan No UPCODE Act, introduced by Senators Cassidy (R-La.) and Merkley (D-Ore.). The first provision would block insurers from inflating risk scores with diagnoses from chart reviews and health risk assessments, unless they are confirmed in a medical setting, and the second would modify the risk adjustment formula to increase parity with traditional Medicare. Combined, these two changes would save $125 billion over 10 years, enough to offset more than half the cost of our PTC proposal. And if lawmakers went further to tackle all the causes of Medicare Advantage upcoding, they could increase their savings to $600 billion, enough to fully pay for our PTC and also begin to address our ballooning federal deficit. Forcing Medicare Advantage plans to boost profits through innovation rather than upcoding could unlock efficiencies from which non-Medicare patients could also benefit.
Expanding the use of site-neutral payments would tackle another perverse incentive currently built into Medicare. Every year, Medicare pays billions more for services performed in a clinic connected to a hospital than it does for similar services performed in a freestanding clinic. One report estimates that payments for preventative exams provided in a hospital outpatient department were 51% higher than payments provided in a freestanding physician’s office.
Since hospital systems still receive higher Medicare reimbursements when providing services in their lower-cost clinic settings, hospital systems are incentivized to buy up freestanding physicians’ offices so they can charge higher reimbursement rates. This swift trend toward consolidation and anti-competitive monopoly structure significantly increases costs to both taxpayers and patients, who are left with fewer cost-effective options for seeking care.
To address this problem, policymakers should work towards equalizing reimbursement rates between outside physician offices and hospital outpatient departments. CMS has some statutory authority to implement site-neutral payment policies and recently proposed ambitious reforms to advance site neutrality as well as other cost-saving measures for beneficiaries. But enacting legislation similar to a bipartisan bill introduced in 2023 would further expand site-neutral payments and could save taxpayers $175 billion over 10 years.
CONCLUSION
Instead of threatening to shut down the government over an outdated pandemic-era program, Democrats should be pressuring Republicans to meet them at a pragmatic middle-ground — one that permanently corrects the structural flaws of the original ACA in a fiscally responsible way. Doing so would signal to the American people that Democrats are serious about cutting medical costs rather than simply increasing government spending. PPI’s fix offers a balanced path forward: scale back the costly and regressive pandemic PTC expansion, smooth the benefit cliff, and pair any new spending with meaningful savings from reducing health-care costs. This combination of targeted assistance and real cost control would deliver more lasting affordability than another costly extension of overpriced subsidies.