President Joe Biden told Americans not to panic about the omicron Covid-19 variant because the U.S. has “the best vaccine in the world, the best medicines, [and] the best scientists.” What the U.S. doesn’t have, however, is the best data. Although the country’s virus DNA sequencing has improved, its data infrastructure still isn’t robust enough to handle this and future pandemics.
When Biden assumed office, the U.S. was sequencing the DNA and thus identifying the viral strains of roughly 8,000 positive Covid-19 tests a week. Ten months later, U.S. labs are sequencing about 80,000 a week. Last week that amounted to one in seven PCR tests. This isn’t enough.
Today, the Innovation Frontier Project (IFP), a project of the Progressive Policy Institute, hosted a virtual conference for policymakers, staffers and journalists titled “How Better Statistics Lead to Better Policy in a Changing World.” The Innovation Frontier Project assembled a panel of leading experts who addressed the need for new statistics in the key areas of the digital economy; healthcare; and supply chains. They showed how a relatively small investment in improving our data can avoid huge policy mistakes.
The high price of insulin for diabetes sufferers has been one of the biggest flashpoints of the drug pricing debate for years. Clearly too many patients struggle with paying for this essential medicine. At the same time, manufacturers claim that the price that they have been receiving for insulin products has been falling.
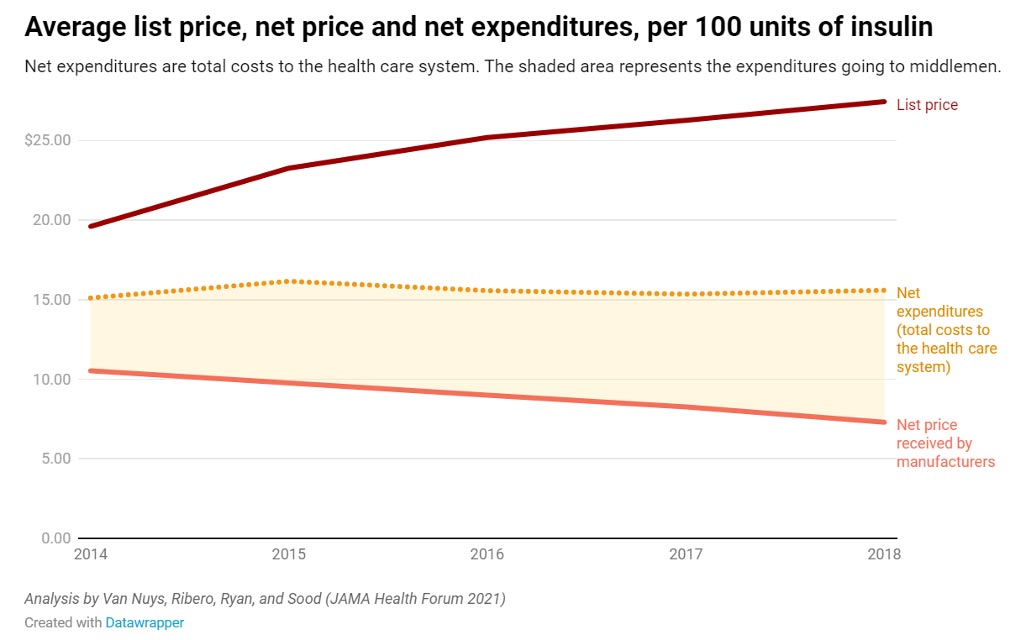
A new study from the USC Schaeffer Center for Health Policy & Economics helps resolve this paradox. The researchers found that middlemen in the distribution process — wholesalers, pharmacies, pharmacy benefit managers (PBMs) and health plans “take home more than half — about 53% — of the net proceeds from the sale of insulin, up from 30% in 2014. Meanwhile the share going to manufacturers has decreased by a third.”
The chart below from the USC report tells the story.
The top line is the list price of insulin, which rose from 2014 to 2018. The bottom line is the net price to manufacturers, which fell over the same period. The middle line is net expenditures to the health care system, which is more or less flat.
This study is completely consistent with anecdotal evidence, suggesting that there’s a growing gap between the list price of insulin and the net proceeds going to manufacturers.
The researchers had to use 15 different data sources to put together their results. They report that:
…Of a hypothetical $100 spent on insulin, they find manufacturers accrued about $70 in 2014, falling to $47 in 2018. During this time, the share going to pharmacies increased from about $6 to $20, pharmacy benefit managers’ share increased from $6 to $14, and the share going to wholesalers increased from $5 to $8. Health plans saw their share decrease from $14 to $10 per $100 spent on insulin.
A single study is not conclusive, of course. But it does suggest that the insulin price problem has as much or more to do with the reimbursement and distribution system as it does with the prices charged by manufacturers. It also raises the need for the government to collect better price statistics that account for discounts and rebates.
While the overarching Build Back Better package remains in limbo until Congress receives a score from the Congressional Budget Office (CBO), it appears that the Democrats have reached a deal on drug pricing. The compromise abandons H.R. 3’s more aggressive components and instead pulls from Senators Ron Wyden and Chuck Grassley’s drug pricing framework.
Democrats worked to thread the needle between progressives’ ambitions to protect seniors from high drug prices and moderates’ desires to protect the incentives to innovate new life savings therapies. They have moved away from initial plans to export drug pricing decisions to other countries — setting a formula based on what other countries had decided drugs are worth. This could have been easily gamed by drug makers but also would have left price decisions up to foreign policymakers instead of making the hard decisions at home.
Instead, the new drug pricing deal would:
Cap seniors’ out-of-pocket costs at $2,000 per year, spread across the year.
Cap insulin costs at $35 per month.
Allow Medicare to negotiate the cost for 10 of the most expensive drugs starting in 2025 increasing to 20 drugs per year by 2028.
Only allow Medicare to negotiate on drugs that have passed an initial market exclusivity period — 9 years for small molecule drugs and 12 years for biologics — addressing market failures when generics don’t create competition and drive down prices.
Use inflation caps in Medicare and the commercial market to limit drug price increases.
Change incentives for Part D insurers to negotiate drug prices more aggressively.
Because these policies will be phased in and are not as draconian as earlier proposals, they may not make a measurable difference to every consumer. But they will undoubtedly help the most vulnerable: seniors with exceptionally high-cost drugs. As PPI has explained in the past, capping out-of-pocket costs and spreading the costs across the year rather forcing seniors to pay huge deductibles up front will make it easier for vulnerable seniors to access lifesaving therapies. PPI has also pushed for reforming incentives for insurance middle-men but those provisions were watered down in the final agreement — instead policymakers settled for increased transparency requirements for pharmacy benefit managers.
This year, the whole world was reminded of the promise of pharmaceutical innovation. Because of the incentives in the U.S. market, Americans had widespread access to COVID-19 vaccines before much of the world. The United States rewards innovation and though the U.S. health care system is worse off on many health are metrics, it out performs other high-income counties on cancer care because of widespread access to new therapies.
Democrats worked together to form a package that preserves incentives to innovate while protecting seniors. We are hopeful that the CBO will provide realistic estimates of the impact the compromise deal that Democrats have coalesced around.
As host of this week’s episode of the Radically Pragmatic Podcast, Progressive Policy Institute (PPI) Director of Health Care Arielle Kane sat down with Charlie Katebi, Policy Analyst at Americans for Prosperity (AFP), to discuss their new bipartisan report “Telehealth Saves Money and Lives: Lessons from the COVID-19 Pandemic.”
“If you imagine over time things leveling out, not having payment parity laws on the books, people more self-selecting into seeking care remotely or in-person, I do think the trend shows that telehealth could garner a bunch of savings. … It shows a lot of potential,” said Arielle on the podcast.
Arielle and Charlie discussed the state of telehealth prior to COVID-19, the potential for cost savings their report identifies, and how policymakers at the federal and state level can confidently take action to protect and expand virtual care.
The podcast and study were in partnership with Americans for Prosperity.
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
When it comes to health policy, “as Medicare goes, so goes the nation.” Unfortunately, burdensome federal regulations prevented Medicare from delivering virtual care to millions of seniors around the country — until the COVID-19 pandemic.
Lawmakers enacted these restrictions because they feared making telehealth widely accessible would lead to patients using unnecessary health care services. Many private insurers followed Medicare’s lead and similarly limited access to many telehealth services.
But when confronted with the crisis of coronavirus, which shut down large parts of the economy and forced families to stay home to reduce the spread of infection, state and federal lawmakers dropped those objections, rightly concluding that telehealth would help people access care during the emergency.
Anew bipartisanreport by the Progressive Policy Institute (PPI) and Americans for Prosperity (AFP) found that over the duration of the pandemic, the costs of telehealth care fell, suggesting that in a post-pandemic world telehealth could help increase access to medical care without increasing costs.
The report, “Telehealth Saves Money and Lives: Lessons from the COVID-19 Pandemic,” analyzed FAIR Health data from January 2020 to February 2021. Its findings contradict assumptions made by the nonpartisan Congressional Budget Office (CBO) that unnecessary health care utilization (i.e. overuse) would increase if telehealth services were made easier to access.
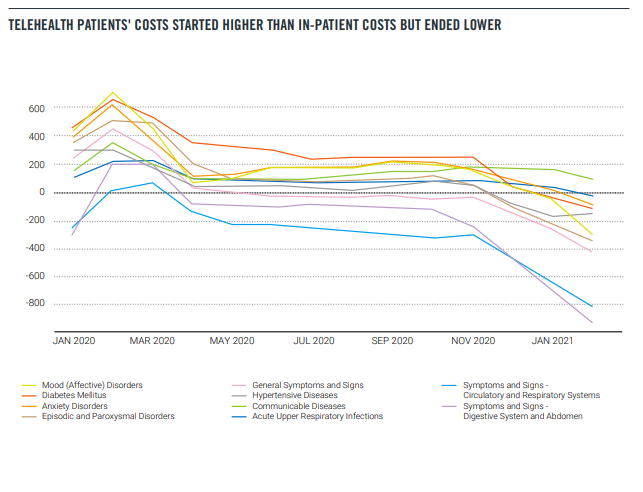
The bipartisan report, authored by PPI Director of Health Care Arielle Kane and Americans for Prosperity Health Policy Analyst Charlie Katebi, found that at the outset of the pandemic, telehealth use skyrocketed, as did costs for those who utilized it versus those who didn’t. But as time went on, the average telehealth patient spent less on health care services than the average in-person patient. In the final month of the study, telehealth patients spent 26% less than the average in-person patient. Further, when excluding the first three months of near complete lockdowns, telehealth patients had lower overall health care utilization.
“Not only does telehealth increase access to care, it also has the potential to be a cost saver,” said Arielle Kane, Director of Health Policy for PPI. “With these findings in mind, policymakers on the federal and state levels can confidently take action to expand access to telehealth services before the emergency provisions expire, protecting services that have directly resulted in patients gaining access to the care they need at a lower cost.”
“Panic over emerging technology is nothing new, but this report shows that the main concerns surrounding virtual care are not supported by evidence,” said Charlie Katebi, Health Policy Analyst at Americans for Prosperity. “Telehealth proved to be a godsend during the pandemic — not just because it kept Americans connected to their doctors, but because it saved them money, too. And while Americans used more virtual care at the height of the pandemic, they used less health care overall. Based on this study, it’s clear that making telehealth more widely available will boost access to quality care and reduce costs.”
The report highlighted recent legislative initiatives aimed at permanently enacting pandemic-era telehealth reforms, including Sen. Brian Schatz (D-Hawaii)’s CONNECT for Health Act and Sen. Joe Manchin (D-W.Va.)’s Protecting Rural Telehealth Access Act. These bills would authorize providers to offer virtual care to Medicare beneficiaries across the country while allowing patients to receive telehealth services at home.
“Ensuring that Americans in rural communities can access the quality healthcare services they need is crucial. My bill, the bipartisan Protecting Rural Telehealth Access Act, gives West Virginians the freedom to attend health care appointments over the phone from the comfort of their homes while also ensuring our healthcare providers are adequately reimbursed. This vital research paper showcases the importance of telehealth services and the potential decreases in individual and taxpayer costs. Increasing awareness on the importance of telehealth services is vital, and I urge my colleagues on both sides of the aisle to support commonsense reforms, like my bill, to ensure every American has access to quality health care, regardless of where they live,” said Senator Manchin.
“Throughout the pandemic, telehealth played a crucial role in ensuring all Americans — particularly seniors and those in underserved communities — could access the health care services they needed, at no risk to themselves,” said Senator Scott. “As this report makes clear, Congress should put the lessons learned from the pandemic into action with appropriate legislation, like the CONNECT for Health Act. Doing so will not only bolster Americans’ access to quality health care today, but it will also ensure that we are better prepared for public health emergencies in the future.”
“Telehealth is a powerful tool in expanding access to quality health care across the country,” Senator Wicker said. “It is encouraging to see momentum grow in the support and utilization of such resources at both the federal and state level. I will continue to champion the permanent expansion of telehealth so that people can continue to use those services, even as we emerge from the coronavirus pandemic.”
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. with offices in Brussels and Berlin. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org and follow PPI on twitter @ppi.
Through broad-based grassroots outreach, Americans for Prosperity (AFP) is driving long-term solutions to the country’s biggest problems. AFP activists engage friends and neighbors on key issues and encourage them to take an active role in building a culture of mutual benefit, where people succeed by helping one another. AFP recruits and engages activists in all 50 states behind a common goal of advancing policies that will help people improve their lives. Learn more at americansforprosperity.org. Join us on Facebook, Twitter, LinkedIn, Instagram and YouTube.
###
Media Contact for PPI: Aaron White – awhite@ppionline.org
Media Contact for AFP: Geoff Holtzman – gholtzman@afphq.org
This report is a joint project of the Progressive Policy Institute and Americans For Prosperity.
INTRODUCTION
Prior to the COVID-19 pandemic, few Americans could access telehealth to meet their health care needs. State and national lawmakers imposed enormous obstacles on patients seeking to virtually connect with their health care provider. Policymakers feared widespread telehealth use would increase spending on unnecessary health care services. As such, Medicare banned clinicians from delivering telehealth outside of rural communities and prohibited patients from receiving telehealth within their homes.
But that dynamic changed when the coronavirus pandemic arrived in the United States, shutting down large parts of the economy and forcing families to stay home to reduce the spread of infection. In early 2020, President Donald Trump declared COVID-19 to be a public health emergency and the federal Department of Health and Human Services (HHS) used its emergency powers to temporarily suspend a variety of regulations to allow Medicare recipients to remotely access care through telehealth. In addition, states waived licensing and regulatory barriers to expand access to virtual care for individuals with commercial insurance.
As a result, telehealth became a safe, reliable source of high-quality care for tens of millions of Americans during the pandemic.
Unfortunately, without codifying these temporary reforms into law, they expire at the end of the public health emergency. The pandemic provides an opportunity to study the impact of the increasing use of telehealth services on health care outcomes and costs. Americans for Prosperity and Progressive Policy Institute worked with FAIR Health to examine how telehealth use changed during the pandemic and assess if it had an impact on costs or health outcomes improved.
Using aggregated, de-identified data from FAIR Health, our study found that while telehealth patients’ costs started higher than in-person patients’ costs, the average telehealth patients’ health care costs fell 61%, from $1,099 per month to $425 per month between January 2020 and February 2021.
Additionally, people who used telehealth had lower overall health care utilization compared with people who used only in-person care, except during the early months of the pandemic, March to May 2020.
Our study confirms a promising trend toward cost savings for patients who use a combination of in-person and telehealth services. These results should give lawmakers confidence to extend the telehealth provisions of the public health emergency rather than letting them expire.
BACKGROUND
There is an axiom in health policy circles: “As Medicare goes, so goes the nation.” Starting in 2001, Congress authorized Medicare to deliver telehealth to the program’s recipients. However, these reforms imposed numerous restrictions that limited the availability of virtual care to a small number of seniors in rural areas. Lawmakers enacted these restrictions because they feared that making telehealth widely accessible would lead to patients accessing unnecessary services. Many clinicians were also hesitant to adopt telehealth, fearing it could disrupt existing practice arrangements and negatively affect their incomes.
But Medicare, insurers, and states shifted their telehealth policies to address COVID-19. On March 13, 2020, President Donald Trump formally declared COVID-19 a national emergency and authorized HHS to temporarily waive laws and regulations to combat and contain the virus. Several days later, Congress passed the CARES Act, which granted HHS additional powers to take emergency measures against COVID-19.
Using its new authority, HHS suspended regulations that prevented health care professionals from remotely delivering care through telehealth. The agency suspended the requirement that Medicare beneficiaries reside in a rural area to receive telehealth services. It waived restrictions that prevented patients from accessing telehealth in their home and allowed for audio-only services. In addition, it permitted rural health clinics (RHCs) and federally qualified health centers (FQHCs) to provide remote virtual care.
HHS also took groundbreaking steps to allow health professionals to deliver a greater array of remote services. The agency announced approximately 240 new telehealth services that providers can deliver to Medicare recipients, including mental health consultations and emergency care.
The agency also authorized all types of health professionals to deliver virtual care to Medicare recipients, expanding the list of telehealth-eligible practitioners to include physical therapists, occupational therapists, and speech language pathologists. Prior to COVID-19, federal law authorized only nine types of health care providers to deliver telehealth services.
Like the federal government, state governors took steps to expand the availability of telehealth to combat COVID-19. Many states suspended regulations that restricted the kinds of technologies practitioners could use to communicate with patients. Ending these restrictions allowed doctors to consult with patients through widely available technology including audio-only phone calls, online video platforms, emails, and instant messages.
Other states waived rules that limited the practice of telehealth to physicians and nurses, expanding practice eligibility to all health care providers licensed by the state. In addition, states removed many rules prohibiting patients from receiving virtual care at home.
Every state also temporarily eased or suspended costly licensing requirements to authorize health care providers licensed in other states to deliver telehealth to their residents. Prior to the pandemic, medical licensing boards charged every license applicant hundreds of dollars and forced them to wait three to nine months before they received a license to practice in their states. These reforms authorized health professionals from all over the country to support patients in pandemic hotspots.
HOW TELEHEALTH CHANGED HEALTH CARE DURING THE PANDEMIC
HHS’s emergency actions expanded access to telehealth for Medicare beneficiaries. Before the pandemic, only 134,000 Medicare enrollees received virtual care every week during the first half of 2019. After these reforms took effect, the number of enrollees receiving telehealth increased over 7,400% to 10.1 million between January and June 2020.
These reforms empowered Medicare patients to access telehealth through an array of technology options that were unavailable prior to the pandemic. Because of the availability of audio-only services, the majority (56%) of Medicare beneficiaries who used telehealth did so via phone. Roughly twice the number of Medicare beneficiaries had a telehealth visit via video (28%).
Removing state and federal barriers also expanded telehealth among individuals with commercial health plans. Prior to the public health emergency declaration in January 2020, providers delivered only 1.5% of health services through telehealth, according to claims data compiled by the COVID-19 Health Care Coalition. After these reforms took effect, providers delivered nearly 24% of all services through telehealth.
These telehealth reforms proved to be especially effective at expanding access for patients with complex conditions. Among Americans with private insurance, another study found that the majority of telehealth users used telehealth for chronic conditions, like diabetes, and behavioral conditions, including depression and anxiety. Another study found physical therapy via telehealth after hip surgery was just as clinically effective and less expensive than in-person care.
Overall, consumer interest in telehealth significantly increased during the pandemic. Prior to the pandemic, consumers were also slow to adopt telehealth. Only 11% of patients had a telehealth visit in 2019. By the height of the pandemic, utilization had increased fourfold. But while the pandemic has kickstarted a dramatic shift in health care delivery, a recent survey found that consumers are increasingly frustrated with limits on telehealth services, opaque costs, and confusing technology requirements.
Additionally, even with the expanded coverage, telehealth services are harder to access in rural areas. Rural Medicare beneficiaries reported that their health care providers were less likely to offer telehealth services than those living in urban areas (52% vs. 67%, respectively). And although telehealth seems like it could help expand the services that small rural hospitals could provide, they are the least likely to have the technology because of the upfront costs. The digital divide affects not only patients but also providers.
WHAT COMES NEXT?
These groundbreaking telehealth reforms are limited to HHS’ COVID-19 public health emergency declaration in early 2020. As soon as the secretary declares the COVID-19 crisis over, these harmful telehealth barriers will resume and patients will lose access to critical virtual care.
Medicare announced it will no longer offer payment parity for video and telephone visits after the federal public health emergency order expires. When it ends, the Medicare Payment and Access Commission (MedPAC) recommended that “Medicare should return to paying the fee schedule’s facility rate for telehealth services and collect data on the cost of providing these services.”
It also calls for ending providers’ discretion to reduce or waive cost sharing for telehealth services. MedPAC also proposed that CMS permanently establish three safeguards after the public health emergency ends to prevent unnecessary spending and potential fraud from telehealth:
Applying additional scrutiny to outlier clinicians who bill significantly more telehealth per capita
Requiring in-person visits before clinicians order expensive medical equipment or laboratory tests
Prohibiting “incident to” billing for telehealth services by clinicians who can bill Medicare
directly
Many states have already reverted to prepandemic telehealth rules. Alaska and Florida have let their public health emergency declarations expire, freezing many telehealth expansions.
However, other states, seeing the value of telehealth, have decided to let telehealth providers keep offering services over the phone pending new federal legislation enabling Medicare to reimburse for a wider spectrum of telehealth services.
TELEHEALTH LEGISLATION
Legislative action is necessary to preserve these essential telehealth reforms. To allow Medicare beneficiaries to access telehealth on a long-term basis, Senator Brian Schatz (D-Hawaii) and a bipartisan group of 59 cosponsors introduced the CONNECT For Health Act.
This bill would permanently extend COVID-era telehealth reforms and allow providers to deliver services to Medicare beneficiaries in every ZIP code in the United States, rather than just rural ones. It would also permit Medicare beneficiaries to receive virtual services from the comfort of their home and authorize important facilities such as Federally Qualified Health Centers and Rural Health Centers to deliver telehealth to patients.
Senator Joe Manchin (D-W.Va.) and other lawmakers introduced a similar bill, the Protecting Rural Telehealth Access Act, which would allow providers to offer virtual care to Medicare patients in any area of the country, permit patients to receive telehealth at home, and authorize FQHCs and RHC to provide virtual care. In addition, it would give Medicare beneficiaries the option to consult with health care providers through audio-only phone calls, video messages, and images, which proved popular during the pandemic.
Senator Tim Scott (R-S.C.) introduced the Telehealth Modernization Act to extend telehealth services to Medicare beneficiaries in any geographic area to receive virtual services, including in the home. Furthermore, it would authorize all types of health care providers to deliver virtual care to Medicare recipients. These measures would preserve the important telehealth reforms HHS implemented during the pandemic that allow providers to deliver medically appropriate virtual care.
DOES TELEHEALTH RAISE COSTS?
While many lawmakers are taking steps to permanently enact telehealth reforms into law, some fear that creating new Medicare telehealth benefits will lead to patients spending more taxpayer dollars on health care. Specifically, skeptics cite analysis from the Congressional Budget Office, which estimates removing Medicare’s telehealth limitations on virtual mental health care would increase utilization and thus spending by $1.65 billion over 10 years.
Fortunately, there is mounting evidence that telehealth can lower health care spending and reduce taxpayer costs. According to a 2021 analysis from the MedPAC, when Medicare patients chose telehealth for their primary care needs, in-person primary care visits fell by 25%.
Virtual care can also decrease health care spending by enhancing preventive care and reducing the need for patients to make expensive visits to hospitals and urgent care centers. One 2012 analysis of the Veterans Health Administration’s telehealth program for chronically ill veterans found virtual care reduced the average cost of every patient by $6,500, saving $1 billion in a single year. The program achieved these savings by reducing hospital admissions by 19% and decreasing the number of days patients spend in the hospital by 25%.
As the pandemic drags on, telehealth continues to prove it enhances patient outcomes and lowers costs. In 2020, Ascension Health found 60% of its telehealth patients would have visited an urgent care clinic or emergency room if they did not offer virtual care. This decreased outpatient visits by 33% for Ascension’s patients.
To expand on this evidence, Americans for Prosperity and the Progressive Policy Institute analyzed aggregated, de-identified data provided by FAIR Health, Inc., based on claims data from its FH NPIC® repository of privately insured medical claims. We received statistical results that reflected the experience of patients who received telehealth and those who did not have any telehealth services. The results also included a nationwide study of telehealth’s effect on patient outcomes and health care spending. Americans for Prosperity and Progressive Policy Institute studied the aggregated data results reflecting the claims experience of 8.1 million patients who used telehealth and compared them to an equivalent aggregated dataset which reflected 15.8 million patients who used inperson care only between January 1, 2020, and February 28, 2021.
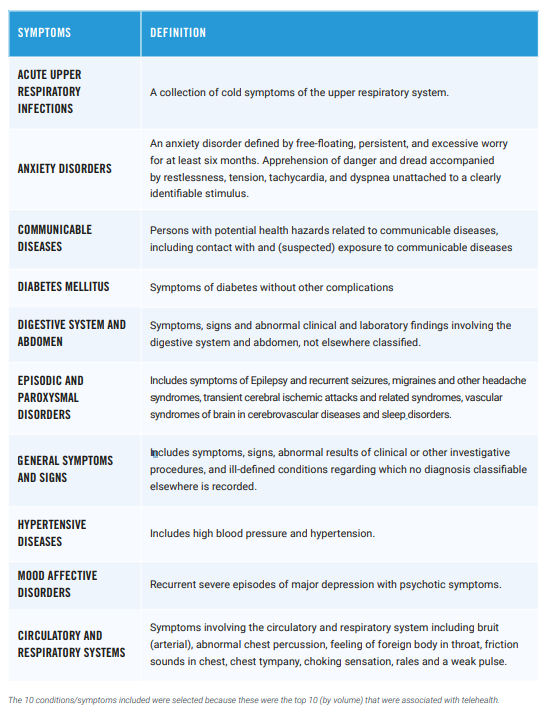
To determine telehealth’s impact on patient outcomes and costs, we compared data from FAIR Health based on de-identified patients of both groups with the same age, sex, and health conditions. The health conditions included mental disorders, hypertensive diseases, communicable diseases, respiratory infections, circulatory and respiratory symptoms, episodic and paroxysmal disorders, digestive system and abdomen symptoms, and diabetes.
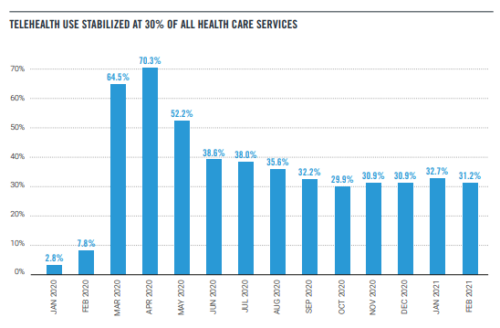
The use of telehealth skyrocketed during the early months of the pandemic. Our study found that in April 2020, telehealth appointments accounted for 70% of all health care appointments.
However, as some of normal life resumed, telehealth appointments stabilized at around 30% of all appointments. Telehealth will never fully replace in-person care, but it’s clear that it can meet patients where they are and help them access needed medical services.
TELEHEALTH PATIENTS’ COSTS
During the pandemic, patients who used telehealth spent more on health services compared with individuals who sought care exclusively from in-person providers. Over the 13-month period studied, individuals who used telehealth spent 19% more on average than in-person patients. This could be explained by the unusual care patterns during the pandemic — sicker patients may have been more afraid of catching COVID-19 and therefore tried to avoid going to the hospital by using telehealth.
Another reason could be policymakers required Medicare, Medicaid, and private health insurers to pay for telehealth services at the same reimbursement rate as in-person services, a policy known as payment parity. Lawmakers intended these measures to encourage providers to offer telehealth as more Americans sought remote care during the pandemic. However, payment parity may have artificially increased the cost of virtual care for patients and taxpayers. Without these expensive mandates, telehealth consultations can cost up to 75% less than in-person consultations. Payment parity may help explain why patients who used telehealth cost more on average than patients who didn’t.
It’s important to note, however, that patients who used telehealth spent significantly less on health services by the end of the study period compared with the start. Between January 2020 and February 2021, the average telehealth users’ monthly health care expenses fell from $1,099 to $425, a 61% decline. Telehealth patients’ costs fell faster than in-person patients: The average in-person patient spent $910 per month in January 2020 and $578 in February 2021.
The data also showed that for seven of the 10 conditions observed, patients who used telehealth spent more than patients who sought in-person care. Only telehealth patients with abdominal symptoms, respiratory symptoms, and general symptoms spent less relative to inperson patients with the same conditions. Again, this could be explained by the unusual care and payment patterns during the pandemic. However, patients of all conditions who used telehealth spent less over time. On a percentage basis, the company found individuals with diabetes, anxiety, and hypertensive diseases had a 71% reduction in spending between January 2020 and February 2021.
TELEHEALTH’S IMPACT ON UTILIZATION
Despite the increased availability of telehealth during the pandemic, for the observed conditions, utilization of the health care system did not increase for telehealth users. For seven of the 10 observed conditions, the average number of total appointments with the health care system — one way to measure utilization — was the same or fewer for people who used telehealth relative to people who did not. The only conditions where utilization was higher were anxiety disorders, mood disorders and communicable diseases. This is easily explained by the fact that anxiety and mood disorders require ongoing care and that the study period included a global pandemic and thus appointments related to communicable disease exposure were high.
In the case of emergency department visits, individuals who used telehealth accessed emergency care more often than individuals who used in-person care. During the 13-month study period, 6% of telehealth patients on average visited the ED per month. In contrast, just 3% of in-person patients accessed emergency care over this period.
But the data showed an important trend line: Individuals who used telehealth made significantly fewer emergency room visits at the end of the study period compared to the start. From January 2020 to February 2021, the average telehealth patient saw their monthly ER visit rate fall from 8.5% to 3.03%. These findings confirm prior research that found telehealth allowed providers to deliver early interventions to individuals, resulting in the use of fewer intensive services.
Taken as a whole, our findings offer strong evidence that the rise of telehealth during the pandemic has not increased overall utilization of the health care system, as many policymakers and budget hawks have feared. While some of the findings will need a longer study window to see what happens after the pandemic ends, it’s evident that consumers don’t use telehealth promiscuously. Instead, telehealth presents a promising opportunity to tailor care to individuals’ unique circumstances and makes it easier for people to access essential services.
CONCLUSION
Our analysis of the aggregated FAIR Health data shows telehealth can dramatically expand health care access without raising costs on taxpayers. Throughout the COVID-19 pandemic, state and federal officials implemented groundbreaking temporary reforms that allowed millions of Americans to remotely access essential care from qualified health professionals. As a result, many policymakers propose making long-term reforms to allow providers to deliver telehealth care on a permanent basis. However, some lawmakers fear that making telehealth available would lead to patients spending more on care by making unnecessary purchases of services.
Our analysis of FAIR Health’s data found patients who use telehealth spend significantly less on health care services over time. Between January 2020 and February 2021, the average telehealth patients’ health care expenses fell 61%, from $1,099 per month to $425 per month. Furthermore, telehealth patients purchased fewer in-person health care services such as emergency care during this time period. This suggests virtual care improves patient health and allows individuals to purchase fewer expensive procedures.
These findings hold important lessons for policymakers in Congress and around the country. Our study shows lawmakers can make important telehealth services widely available to families without raising costs on taxpayers. Therefore, Congress should permanently empower health practitioners to provide virtual care to all Medicare recipients. This would ensure seniors continue to receive quality and cost-effective care from the convenience of their homes long after the pandemic ends.
ABOUT THE AUTHORS
Arielle Kane is the director of Health Policy at the Progressive Policy Institute. Her research focuses on what comes next for health policy in order to expand access, reduce costs and improve quality.
Charlie Katebi is a health policy analyst for Americans for Prosperity, where he promotes state and federal policies that increase patient choices, lower costs, and expand access to quality health care.
There is a massive amount of wasteful spending in healthcare. Credible research suggests that roughly one-quarter of our total healthcare spending is wasted on low-value care, administrative complexity, including prior authorization processing, and failure of care delivery.
However, there is at least one area in healthcare that is indisputably high value: vaccines. Vaccines are widely regarded as the most cost-beneficial intervention in healthcare. Unfortunately, and counterintuitively, current cost-sharing policies discourage our most vulnerable population – seniors – from accessing vaccines.
Most private insurance policies or Affordable Care Act (ACA) plans provide coverage for vaccines without any out-of-pocket cost to the patient to encourage patients to be vaccinated. Regrettably, the same cannot be said for Medicare. Medicare coverage of vaccines for seniors is a tale of two cities. Vaccines paid for through Medicare Part B that are recommended by the Advisory Committee on Immunization Practices (ACIP) require zero out-of-pocket costs for patients. However, newer vaccines recommended by ACIP, except those for COVID-19, are covered under the Medicare Part D benefit and require an out-of-pocket expense for the beneficiary that can range from a few dollars to the entire cost of the vaccine.
Join PPI Senior Fellow for Health Policy Robert Popovian on November 2nd, 2021 at 1:00pm ET for a panel hosted by State of Reform on innovative strategies to reduce health care costs – which could include formulary adjustments, strategies to increase the use of biosimilars, or other creative policy solutions.
The pandemic has shifted the politics and public opinion on health care. Where cost was a primary concern before COVID, now access to affordable innovations is top of consumers and policy makers minds. So, as a return to normalcy appears on the horizon, the intersection of cost pressures and innovation in pharmacy is becoming a primary topic of concern in health policy.
Panelists:
Robert Popovian, PharmD: Senior Fellow, Health Policy, Progressive Policy Institute
Sarah Ikenberry: Senior Communication Advisor, Therapeutic Biologics and Biosimilars
Kashyap Patel, MD: President, Oncology Care Alliance
Menstrual products are as necessary as toilet paper and soap. Yet, one in four women and girls in the U.S. struggle to pay for them. This lack of access to these products amongst school-aged female students directly impacts the quality of their education and well-being. A 2021 study conducted by the University of Pennsylvania found that 80% of female students have missed all or part of a class or know someone who had to miss class because they did not have access to menstrual hygiene products. Implementing programs that provide no-cost menstrual hygiene products in all public school restrooms will benefit girls’ education, especially for students of color and those with a lower-income background who tend to be more impacted by this issue.
“Period poverty.” or the inability to afford and lack access to menstrual and sanitary products, can also worsen the social stigma around menstruation. Cultural shame attached to menstruation and a shortage of menstrual hygiene resources prevents many women and girls from carrying out their daily routines. Without constant, reliable access to menstrual products at school, students are forced to ask the school nurse or their friends, who might only have a limited supply of products. Some prefer to skip classes entirely because of the discomfort of not having access to these products. All of these disruptions can lead to learning loss and educational barriers for female students.
Beyond impacting education, period poverty can also affect students’ mental and physical health. Roughly 68% of students who experienced monthly period poverty reported moderate to severe depression. Furthermore, researchers found that 50% of students who could ill afford to buy the disposable products, in an effort to stretch their dollars, did not change them out every four to eight hours as recommended by the Food and Drug Administration. This increases the risk of a rare but deadly reaction known as “Toxic Shock Syndrome” and other bacterial infections.
There is momentum across the country to address this issue. Currently, legislation to make menstrual hygiene products available in all public school restrooms has passed in states such as Rhode Island, Nevada, Washington, and California. This past May, Congresswoman Grace Meng (D-N.Y.) introduced the federal Menstrual Equity for All Act of 2021 (H.R. 3614) that would require public elementary and secondary schools to provide free menstrual products for its students by amending the Elementary and Secondary Education Act of 1965.
Young women across the country deserve to attend school without fear or shame about how menstruation might impact their education and health. Policymakers at the state and federal level should work to ensure that there are free or affordable menstrual products available in all public school bathrooms so that our most vulnerable female students can go about their school day without interruptions or social stigma.
As the cost of President Joe Biden’s spending package shrinks from $3.5 trillion closer to $2 trillion, Senator Bernie Sanders’s proposal to add dental, vision and hearing coverage to Medicare has emerged as a sticking point in negotiations. Opposing Sanders are Democrats such as Congressman Jim Clyburn of South Carolina who would like to prioritize spending to benefit low-income people — including by providing health insurance for the poor in states that have refused to expand Medicaid.
There is a way to compromise — to add new benefits to Medicare without spending so much that there’s no room in the budget for helping the Medicaid-deprived.
Rather than simply offer dental, vision and hearing benefits to all Medicare beneficiaries, create an optional, buy-in policy. This would enable seniors to take advantage of the federal government’s purchasing power but still limit the cost to taxpayers. It would keep Medicare solvent longer. And it would provide standardized plans for beneficiaries — rather than the patchwork of coverage now available to those who sign up for Medicare Advantage or supplemental Medicare plans.
Older Americans clearly need affordable dental, vision and hearing coverage. The only question is how best to pay for it. A buy-in program could be structured like the Affordable Care Act and the Medicare Part D prescription drug benefit, both of which give subsidies to people below a certain income threshold.
Rather than cutting corners and using gimmicks to cram the entire progressive wish list into a smaller bill, PPI believes the party’s goal should be a more focused and disciplined reconciliation bill that sets clear priorities and accomplishes a few big objectives well. Specifically, this report outlines a bold plan to deliver on three urgent priorities of the Democratic party within the confines of a roughly $2 trillion bill: supporting working families, combating climate change, and expanding access to affordable health care for those in need.
“Despite the drama last week, President Biden and Democrats in Congress can still deliver the historic economic and social investments they promised during the campaign — but they need to spend smarter, not just bigger. Our blueprint is a reality-based approach to crafting the reconciliation bill, which will allow for an enormous advance of progressive government. Now is the time for the party to come together and show America they can govern,” said Ben Ritz, Director of the Center for Funding America’s Future.
“We urge Democrats to compromise around a set of urgent priorities the American people can understand, develop a consensus plan to fully pay for it, and work in a radically pragmatic spirit to get this big progressive win across the finish line. That’s the best way to help President Biden and their party deliver for the American people,” said Will Marshall, President of the Progressive Policy Institute.
The bipartisan infrastructure bill passed by the U.S. Senate in August remains snagged by internal disagreements among Congressional Democrats about the size and cost of the follow-on social investment package party leaders hope to pass with reconciliation rules that are not subject to a Republican filibuster. Democrats will likely need to reach a compromise on the reconciliation package by October 31st so they can pass the infrastructure bill before funding for the nation’s highway program expires.
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
Launched in 2018, PPI’s Center for Funding America’s Futureworks to promote a fiscally responsible public investment agenda that fosters robust and inclusive economic growth. We tackle issues of public finance in the United States and offer innovative proposals to strengthen the foundation of our economy and build shared prosperity.
The White House and Congressional Democrats are at a pivotal moment in their long-running effort to turn President Biden’s ambitious “Build Back Better” vision into law. The bipartisan infrastructure bill passed by the U.S. Senate in August remains snagged by internal disagreements among Congressional Democrats about the size and cost of the follow-on social investment package party leaders hope to pass with reconciliation rules that are not subject to a Republican filibuster. Democrats will likely need to reach a compromise on the reconciliation package by October 31st so they can pass the infrastructure bill before funding for the nation’s highway program expires.
Though cast as a power struggle between the progressive left and the pragmatic center, what’s happening on Capitol Hill is actually a reconciliation with legislative reality. Democrats can only afford to lose three votes in the House of Representatives and have no margin of error in the Senate, where at least two Members, Sens. Joe Manchin, D-W. Va., and Kyrsten Sinema, D-Ariz., already have made it clear they won’t support a $3.5 trillion bill. Many Democrats in the House have concerns as well. Accordingly, President Biden says negotiators are now aiming for a final package that will likely cost between $1.9 trillion and $2.3 trillion.
Some progressives are trying to make their whole wish list fit within this budget constraint by setting arbitrary dates for programs to expire, as Republicans did to disguise the true cost of their 2001, 2003, and 2017 tax cut bills. For example, rather than spend $225 billion every year in the 10-year window, the package envisioned by the left might spend $450 billion each year for five years before abruptly expiring.
But this approach would be deeply problematic. As Rep. Ron Kind, D-Wisc., noted in a recent op-ed, “funding programs for two to three years at a time only creates uncertainty and unnecessary fiscal cliffs.” In the worst-case scenario, a Republican Congress could allow programs to expire, which would upend the Biden legacy while pulling the rug out from people who planned their lives around new benefits.
Rep. Suzan DelBene, D-Wa., chair of the moderate New Democrat Coalition in the House, further explained why such a package wouldn’t alleviate the fiscal concerns of many pragmatic Democrats: “If you assume that you’re going to do something short term just to make it look like it’s going to fit in a particular budget window, for a particular piece of legislation, but you assume it’s going to be renewed later, then you aren’t really being honest about what your long-term budget goals are.”
Fortunately, Democrats can still deliver historic economic and social investments that the country needs by spending smarter, not just bigger. The goal should be a more focused and disciplined reconciliation bill that sets clear priorities and accomplishes a few big objectives well instead of haphazardly trying to do everything at once. Specifically, PPI believes that lawmakers should focus on delivering three urgent priorities effectively: supporting working families, combating climate change, and expanding access to affordable health care for those in need. As President Biden has promised, the package should also be fully paid-for with credible offsets.
There can be no doubt that a bill along these lines would constitute an enormous advance for progressive government. When combined with the $1.9 trillion American Rescue Plan and the $550 billion bipartisan infrastructure bill, this package would represent the third pillar of the largest and most progressive public investment since the Great Society over 50 years ago. These landmark legislative accomplishments would constitute a clear and indisputable victory for President Biden’s vision and a win for Democrats of all stripes.
Here’s what a roughly $2 trillion package should include:
Supporting Working Families ($975 billion)
The American Rescue Plan increased the value of the Child Tax Credit and made the full value of the credit available to low-income families for the first time ever. This policy change has helped cut child poverty in half for 2021 and directly empowered parents to support their children without having to rely on siloed and difficult-to-access welfare bureaucracies. PPI has previously proposed a framework for making the full expansion permanent that would cost just over $800 billion. However, Congress could adopt a smaller expansion of the CTC and redirect the funds for other programs that support working families. This approach is sensible because making the CTC fully available to low-income families both does more to reduce poverty and costs less than increasing the CTC’s total value.
In addition to permanently expanding the CTC, Democrats should invest in our children’s education by making preschool, which is shown to dramatically increase a child’s lifetime earnings, universally available to three- and four-year olds. The cost of universal preschool should be reduced by either means-testing it or requiring high-income school districts to help cover the cost of this program.
PPI also believes Washington should stop underinvesting in non-college workers by creating multiple pathways to middle-class jobs, including new investments in apprenticeships and “last mile” job training initiatives. Finally, lawmakers could offer new parents a flat paid parental leave benefit that future Congresses could expand into a full paid family and medical leave program if they are willing to consider a broader menu of offsets to pay for it.
Combating the Climate Crisis ($600 billion)
The bipartisan infrastructure bill that passed the Senate in August offered a strong down payment on tackling the climate crisis, including funding for public transit, energy grid modernization, and carbon capture demonstration projects, but far more needs to be done. The follow-up bill should include a package of well-designed tax credits similar to the one produced by the Senate Finance Committee that would encourage the adoption of affordable electric vehicles and other green technologies. It should also fund meaningful climate resilience projects and additional investments in breakthrough technologies such as carbon capture, hydrogen energy, geothermal energy, and advanced nuclear power.
Another top priority is the Clean Energy Payment Program (CEPP) that would provide subsidies for electric utilities that increase the share of clean energy they produce by 4% each year while charging smaller penalties for those that do not. These provisions could be responsible for almost two-thirds of the emissions reductions sought by President Biden. However, the CEPP has run into concerns from Sen. Manchin and it may run afoul of the Byrd rule that governs what policies can be passed through the reconciliation process that allows Democrats to circumvent a Republican filibuster.
Climate change poses a large and growing threat to our economy, so even if the CEPP cannot be included in the package, it must be replaced by another policy to accomplish the same objective. PPI has long advocated for a carbon tax, possibly paired with rebates to mitigate the burden on low- and middle-income families. Some portion of the revenue could also be earmarked for funding additional investments in research and development to promote innovation and technology growth.
Strengthening the Affordable Care Act ($425 billion)
Some progressives in Congress, led by Sen. Sanders (I-Vt.), insist that America’s top health care priority should be expanding Medicare to cover dental, hearing, and vision benefits, which would cost more than $800 billion in the 10-year period after being fully phased-in. But it hardly seems “progressive” to provide more generous coverage for Medicare beneficiaries when millions of Americans have no health coverage at all — especially considering that the majority of seniors already have coverage for these services through Medicare Advantage or supplemental Medigap plans.
Instead, PPI believes Democrats should back Speaker Pelosi’s call for building on the Affordable Care Act by making some share of the American Rescue Plan’s expansion of insurance subsidies for middle-income households permanent and by providing coverage to the more than 2.2 million uninsured people who should be eligible for Medicaid in the 12 states that have yet to expand the program. These provisions to expand coverage should also be paired with policies to address the out-of-control growth of health care costs, such as price caps or a national public option, to both reduce the net cost of these provisions and make health care more affordable for all Americans. Any expansion of Medicare should be fully financed by income-based premiums or dropped altogether so it does not draw critical resources away from the other priorities in this package.
Conclusion
In addition to the Sanders Medicare expansion, PPI’s reconciliation framework omits some major elements of Biden’s original Build Back Better blueprint, including more public support for child and elder care, community colleges, and more. Their absence here doesn’t necessarily mean these priorities are unworthy of Democrats’ support, but rather reflects the political imperative of fashioning a compromise package that can unite the party’s diverse coalition. It is also critical that lawmakers avoid the temptation to waste limited funds on other parochial priorities, such as cutting taxes for their rich constituents by weakening or repealing the SALT cap, when so many more-worthy priorities are left unfulfilled.
Passing both the infrastructure and social investment bills has become a critical test of Democrats’ ability to govern. We urge Democrats to compromise around a set of urgent priorities the American people can understand, develop a consensus plan to pay for it, and work in a radically pragmatic spirit to get this big progressive win across the finish line. That’s the best way to help President Biden and their party deliver for the American people.
Ben Ritz is the Director of PPI’s Center for Funding America’s Future. He previously staffed the Bipartisan Policy Center’s Economic Policy Project and served as Legislative Outreach Director for The Concord Coalition. Ben earned his Master’s of Public Policy Analysis and a Graduate Certificate of Public Finance from American University, where he also previously completed his undergraduate education. Follow him on Twitter: @BudgetBen
About the PPI Center for Funding America’s Future:
The PPI Center for Funding America’s Future works to promote a fiscally responsible public investment agenda that fosters robust and inclusive economic growth. We tackle issues of public finance in the United States and offer innovative proposals to strengthen the foundation of our economy and build shared prosperity.
The COVID-19 virus is endemic — meaning it’s here to stay. Getting to a 70% or 80% vaccination rate will not stop breakthrough cases, hot spots, and vulnerable people from getting ill. As such, the United States needs to pivot its COVID-19 response strategy to focus on harm reduction to prevent unnecessary deaths without forcing people to live another year in lockdown limbo.
To do that, the U.S. can learn from other countries with fewer cases and deaths.
We need to vaccinate as many people as possible.
The United States needs to continue to vaccinate as many people as possible, including eligible children, hard to reach and underserved populations, and the vaccine hesitant. The federal worker vaccine mandate should push more people to get vaccinated, but rollout efforts should not stop there. Music venues, sporting arenas, and schools can all encourage more people to get vaccinated by requiring proof of vaccination for entry. Having vaccines available during large events could also help reach some people.
We need more testing.
The United States has roughly the same vaccination rate as Germany and France and yet they have far fewer cases. A big reason is because they have prolific, and subsidized, COVID-19 testing — though Germany just recently stopped offering free COVID-19 tests to unvaccinated adults. In the U.S., rapid tests should be readily available for people with cold symptoms, people in schools, people who work in congregant settings, and people who want to travel. In the U.K., France, and Germany, rapid testing is widely available and inexpensive. People should get tested before gathering and traveling, which helps keep transmission down.
In general, the U.S. Food and Drug Administration (FDA) has been slow to approve rapid, at-home tests because they are less accurate than PCR tests. Because it has only approved a handful of rapid tests, they are expensive and often sold out at local pharmacies. If getting a PCR test requires an appointment and has a 2-5 day turn around, people aren’t going to use them as a mitigation strategy. The government should approve more rapid tests — even if they aren’t as effective as PCR tests — so that widespread use is easy and affordable.
Kids need to be in school as much as possible.
After a year and a half of closures and remote learning of uneven quality for many children, it is paramount that they stay in school. Children who are exposed to infected people should not be forced to stay home if they are vaccinated. Exposed unvaccinated children should be tested and stay in school unless they test positive. As vaccines become available for school-aged children, they should get vaccinated against COVID-19 as they are against other diseases. Local policymakers should work on appropriate vaccine mandates for school and school-related activities.
We need early access to treatments.
When someone tests positive, they should know where they can get treatments as quickly as possible to reduce the likelihood of hospitalization, particularly if they are more vulnerable. Research from Baylor University Medical Center found that monoclonal antibodies reduced hospitalizations among high-risk COVID-19 patients if they received the therapy early in the course of their illness. This means that doctors need to be aware of and prescribe the treatment and patients need access to infusion facilities since the drugs are delivered intravenously within the first 10 days of symptoms. But many primary care providers don’t know where to direct people to receive treatment. The federal government has announced that it will work on more equitably distributing the limited supply of monoclonal antibody treatments. But they should work with local governments and state medical boards to better reach vulnerable patients who test positive.
Everyone needs insurance coverage.
While the uninsured rate largely remained unchanged during the pandemic, where people were getting their coverage from changed. As people lost their jobs, more people enrolled in Medicaid. This prevented a huge loss of coverage. But in Republican-dominated states that haven’t yet expanded Medicaid under the Affordable Care Act (ACA), the rate of uninsured remains much higher than the national average. The data shows that access to health insurance coverage improves health outcomes, because covered people are more likely to get preventive care and earlier interventions when they need acute care. One study found that COVID cases and deaths are higher in non-expansion states, suggesting that Medicaid improves access to health care system and limits both the rates of transmission and death.
In the reconciliation negotiations, lawmakers should prioritize covering the roughly 2.2 million Americans would be eligible for Medicaid save for the fact that they live in one of the 12 states that have elected to forgo Medicaid expansion under the ACA. Congress should work to plug that hole in a cost-effective manner that does not disadvantage the states that elected to expand Medicaid. Medicaid expansion has been linked to fewer bankruptcies and better health outcomes.
We need good paid leave policies.
To limit the spread of infection, the expectation is that people stay home from work when they test positive. This means that people shouldn’t fear losing their job or being unable to pay the bills if they get COVID. To protect workers, we need better sick leave policies. In the U.S., 95% of the highest earning 10% of private employees have paid sick leave, while only 33% of the lowest earning 10% of private employees had paid sick time leave. Given that the virus disproportionately affects low-income people, the U.S. needs to standardize sick leave policies to protect all Americans.
We need to reduce poverty.
Compared to other high-income countries, the U.S. has the worst health outcomes. And while there are many problems with the health care system that make it expensive, difficult to navigate, and otherwise dissuade people from getting needed care, the main reason the U.S. has poor outcomes is because we underinvest in other social determinants of health. If the U.S. invested more in social services for children and working-age adults, it is likely it could close the gap between the U.S. and other high-income countries. More equitable access to good nutrition, education, child care, housing, transportation, and worker benefits helps people live healthier lives that can mitigate the impacts of COVID-19. Poverty rates fell during the early stages of the pandemic because of generous unemployment benefits and stimulus payments. The U.S. should continue efforts to reduce poverty and improve social determinants of health.
With vaccinations, naturally acquired immunity, and other mitigation efforts, COVID-19 is morphing from an acute pandemic to an endemic condition like seasonal flu. But the U.S. can do a much better job reducing infection and death rates. These commonsense steps will protect vulnerable Americans without the need for lockdowns, school closures, and extensive social distancing which made life so difficult over the last 1.5 years.
By Dr. Michael Mandel, Chief Economic Strategist; and Dr. Robert Popovian, Senior Fellow at PPI
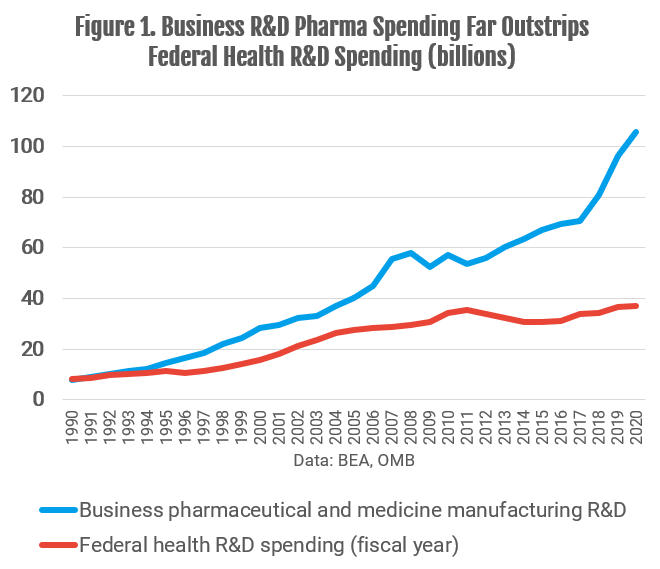
As Congress is considering the shape of the $3.5 trillion reconciliation bill, one of the biggest flash points is drug pricing reform. Drug price reform is very popular, but when you look closely at the data, as we did in our February 2021 report, the evidence for out-of-control drug price increases becomes much less compelling. Spending on drugs, net of rebates and discounts, is basically flat as a share of GDP over the past decade. At the same time, the pharma industry has boosted spending on R&D much faster than the federal government. In 2020, the U.S. pharma industry spent $106 billion on R&D, almost triple the $37 billion in health R&D coming from the federal government (Figure 1).
Equally important, pharma manufacturers’ revenue, net of discounts and rebates, increased by only 11%, or $36 billion, between 2016 and 2020, according to a report from the IQVIA Institute. Taking the industry as a whole, all of that revenue gain went into increased R&D spending.
That’s not to say that some people aren’t hurting. In 2018, only 1 percent of Americans paid more than $2,000 in out-of- pocket drug expenses, not including Part D premiums, according to our analysis. That’s a small percentage, but a significant number of people in the aggregate.
Moreover, data analyzed by PPI and others suggest that the major issue irritating most American families is the insane number of copays that people have to pay as they get older. On average, the typical American between the ages of 50 and 60 fill almost thirty prescriptions per year, while the typical American over 65 and over fill almost 50 prescriptions per year. Most drugs are covered by insurance, but even when each copay is small, these numbers add up quickly and are a growing drag on household budgets. In an October 2019 report, we call this the prescription escalator, since the number of prescriptions — and copays — rises sharply with age.
The problem is that the centerpiece of the drug pricing reform proposal–broad Medicare drug price negotiation–will almost definitely hurt R&D and new drug development without actually addressing most of the co-pays that Americans pay. A recent CBO study estimates that drug price reform (similar to what has been proposed) would lead to 59 fewer new drugs over the next three decades. Moreover, key lines of drug development may never even be funded, leading to missed opportunities for saving lives and reducing medical costs in the future. That’s unfortunate, coming after a year when the industry outperformed the rest of the world by developing “gold standard” vaccines in record time.
Given the current levels of R&D spending, excessively squeezing the revenues received by pharma companies will inevitably translate into fewer new drugs. That implies Democratic Representatives Scott Peters (D-Calif.), Kathleen Rice (D-N.Y.) and Kurt Schrader (D-Ore.), who voted against the drug pricing proposal in the House Energy and Commerce Committee markup process, have solid grounds for worrying that such legislation will undercut investment in innovative drugs.
The drug pricing proposal being considered does contain some good features, including reforming Medicare Part D to cap catastrophic spending. But from a political perspective, it should also deal with the prescription escalator problem that is a key driver of the negative feelings towards drug prices. That means capping out-of-pocket drug expenses, not just for Medicare Part D but for all medical insurance. We examined this in our February 2021 report, “Memo to President Biden: A Reality-Based Approach to Drug Pricing.” In that paper, we support a cap on out-of-pocket costs for drugs, including copays, similar to legislation proposed in 2018. We also support a shift to point-of sales rebates, which should benefit consumers and align their incentives with actual net prices. Getting more transparency into the system is essential.
Finally, we need a better payment scheme for new drugs, especially potential cures for major diseases that are socially beneficial and cost-saving over the long run, but expensive to develop. The most straightforward solution is a shift to outcome-based pricing, which will get new drugs to market faster while having the pharma companies absorb more of the risk.