As host of this week’s episode of the Radically Pragmatic Podcast, Progressive Policy Institute (PPI) Director of Health Care Arielle Kane sat down with Charlie Katebi, Policy Analyst at Americans for Prosperity (AFP), to discuss their new bipartisan report “Telehealth Saves Money and Lives: Lessons from the COVID-19 Pandemic.”
“If you imagine over time things leveling out, not having payment parity laws on the books, people more self-selecting into seeking care remotely or in-person, I do think the trend shows that telehealth could garner a bunch of savings. … It shows a lot of potential,” said Arielle on the podcast.
Arielle and Charlie discussed the state of telehealth prior to COVID-19, the potential for cost savings their report identifies, and how policymakers at the federal and state level can confidently take action to protect and expand virtual care.
The podcast and study were in partnership with Americans for Prosperity.
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
A terse description of a high-seas pirate attack off Nigeria three weeks ago, from the International Maritime Bureau’s Piracy Reporting Centre:
Oct. 25, 2021: While underway, a container ship was boarded by an unknown number of pirate and the crew retreated into the citadel. On being notified of the incident, the IMB Piracy Reporting Centre immediately alerted and liaised with the Regional Authorities and international warships to request for assistance. A Russian Navy warship and its helicopter responded and proceeded to render assistance resulting in the crew and ship being safe. The pirates escaped with stolen ship’s properties.
Background: A decade of naval cooperation, even among distrustful big powers, appears to have made high-seas pirate work more difficult and less rewarding.
In 2010, international waters off Somalia — the Red Sea, the Gulf of Aden, and the ‘Bab-el-Mandeb’ strait, the principal commercial and energy link between Asia and Europe, with 50 ship transits and 3.4 million barrels of oil moving daily — were the center of the pirate industry. The collapse of Somalia’s central state in 1991 left country prey to sequential waves of violent clan-based militias, radical fundamentalists and crime gangs. One product of this was a notorious high-seas pirate industry; at its peak from 2005 to 2010, gangs using small speedboats and automatic weapons were attacking three or more ships a week on the high seas — in total, 181 attacks in 2009 — and in 2010 they were holding 30 vessels and 600 sailors for ransoms ranging up to $95 million.
Since then, the 29-country naval patrol known as CTF-151 (“Combined Task Force 151”) with rotating commands led this year by Pakistan and now Brazil, appears to have essentially eliminated the Somali pirate industry. The last two successful attacks on high-seas vessels in this region were in 2017, and the most recent failed attempt was in 2019; none at all are reported for 2020 and 2021.
On a worldwide scale, pirate attacks have fallen by over half in the past decade, from 445 known attacks in 2010 to 195 in 2020. The running tally kept by the International Maritime Bureau in Kuala Lumpur suggests that this year’s count may fall below 150, which would be the fewest attacks since 1994. Piracy is now most frequent in Indonesia and in the Singapore Strait, the sites of 47 of last year’s 161 attacks and 25 of the 97 attacks reported through September 2021. Only two of these, though, were actual attacks on high-seas shipping; the others were attempted robberies of ships in port or at anchor. Attacks off West Africa are somewhat less frequent — 24 in 2020, or two each month — but appear to feature especially well-armed and violent pirates, responsible for all three 2020 high-seas hijackings of ships, along with 128 of the 135 crew kidnappings, and nine of the 11 incidents of firing on shipping. In West Africa too though, frequency and severity have diminished this year, with the open-water event off Brass last month the only high-seas attack recorded so far. Its quick interruption by a Russian naval patrol, even though the pirates got away with some stolen equipment, suggests some success for international naval cooperation here as well.
FURTHER READING
Facts and data
The International Maritime Bureau’s piracy reports for 2020 find:
Totals: 195 pirate attacks of all kinds worldwide, down from a peak of 445 attacks in 2010, and down again by 30% (from 132 to 97) through the first nine months of 2021.
Hijackings: 11 hijackings of high-seas shipping, down from 53 in 2010; only two so far in 2021.
The International Maritime Bureau on recent pirate attacks, with the full-year 2020 and partial-year 2021 reports available at no cost via e-mail:
Navy perspectives
Command Task Force 151, led last year by Pakistan and this year by Brazil, patrols Somali waters.
And the U.S. Navy reports on joint anti-piracy training with the Ghanaian navy this spring, and Ghanaian-American sailors Samuel Ellis and Prince Boateng visiting home.
The Singapore-based Information Sharing Center for the Regional Cooperation Agreement on Combating Piracy (RECAAP) oversees anti-piracy operations in maritime Southeast Asia.
Two views on Somali piracy
Brookings Institution scholars speculate on a link between illegal/unreported/unregulated fisheries and piracy rates, can be read here.
And a personal account from journalist Michael Scott Moore in The Guardian, on his 977 days as a pirate kidnap victim can be read here.
ABOUT ED
Ed Gresser is Vice President and Director for Trade and Global Markets at PPI.
Ed returns to PPI after working for the think tank from 2001-2011. He most recently served as the Assistant U.S. Trade Representative for Trade Policy and Economics at the Office of the United States Trade Representative (USTR). In this position, he led USTR’s economic research unit from 2015-2021, and chaired the 21-agency Trade Policy Staff Committee.
Ed began his career on Capitol Hill before serving USTR as Policy Advisor to USTR Charlene Barshefsky from 1998 to 2001. He then led PPI’s Trade and Global Markets Project from 2001 to 2011. After PPI, he co-founded and directed the independent think tank ProgressiveEconomy until rejoining USTR in 2015. In 2013, the Washington International Trade Association presented him with its Lighthouse Award, awarded annually to an individual or group for significant contributions to trade policy.
Ed is the author of Freedom from Want: American Liberalism and the Global Economy (2007). He has published in a variety of journals and newspapers, and his research has been cited by leading academics and international organizations including the WTO, World Bank, and International Monetary Fund. He is a graduate of Stanford University and holds a Master’s Degree in International Affairs from Columbia Universities and a certificate from the Averell Harriman Institute for Advanced Study of the Soviet Union.
When it comes to health policy, “as Medicare goes, so goes the nation.” Unfortunately, burdensome federal regulations prevented Medicare from delivering virtual care to millions of seniors around the country — until the COVID-19 pandemic.
Lawmakers enacted these restrictions because they feared making telehealth widely accessible would lead to patients using unnecessary health care services. Many private insurers followed Medicare’s lead and similarly limited access to many telehealth services.
But when confronted with the crisis of coronavirus, which shut down large parts of the economy and forced families to stay home to reduce the spread of infection, state and federal lawmakers dropped those objections, rightly concluding that telehealth would help people access care during the emergency.
Anew bipartisanreport by the Progressive Policy Institute (PPI) and Americans for Prosperity (AFP) found that over the duration of the pandemic, the costs of telehealth care fell, suggesting that in a post-pandemic world telehealth could help increase access to medical care without increasing costs.
The report, “Telehealth Saves Money and Lives: Lessons from the COVID-19 Pandemic,” analyzed FAIR Health data from January 2020 to February 2021. Its findings contradict assumptions made by the nonpartisan Congressional Budget Office (CBO) that unnecessary health care utilization (i.e. overuse) would increase if telehealth services were made easier to access.
The bipartisan report, authored by PPI Director of Health Care Arielle Kane and Americans for Prosperity Health Policy Analyst Charlie Katebi, found that at the outset of the pandemic, telehealth use skyrocketed, as did costs for those who utilized it versus those who didn’t. But as time went on, the average telehealth patient spent less on health care services than the average in-person patient. In the final month of the study, telehealth patients spent 26% less than the average in-person patient. Further, when excluding the first three months of near complete lockdowns, telehealth patients had lower overall health care utilization.
“Not only does telehealth increase access to care, it also has the potential to be a cost saver,” said Arielle Kane, Director of Health Policy for PPI. “With these findings in mind, policymakers on the federal and state levels can confidently take action to expand access to telehealth services before the emergency provisions expire, protecting services that have directly resulted in patients gaining access to the care they need at a lower cost.”
“Panic over emerging technology is nothing new, but this report shows that the main concerns surrounding virtual care are not supported by evidence,” said Charlie Katebi, Health Policy Analyst at Americans for Prosperity. “Telehealth proved to be a godsend during the pandemic — not just because it kept Americans connected to their doctors, but because it saved them money, too. And while Americans used more virtual care at the height of the pandemic, they used less health care overall. Based on this study, it’s clear that making telehealth more widely available will boost access to quality care and reduce costs.”
The report highlighted recent legislative initiatives aimed at permanently enacting pandemic-era telehealth reforms, including Sen. Brian Schatz (D-Hawaii)’s CONNECT for Health Act and Sen. Joe Manchin (D-W.Va.)’s Protecting Rural Telehealth Access Act. These bills would authorize providers to offer virtual care to Medicare beneficiaries across the country while allowing patients to receive telehealth services at home.
“Ensuring that Americans in rural communities can access the quality healthcare services they need is crucial. My bill, the bipartisan Protecting Rural Telehealth Access Act, gives West Virginians the freedom to attend health care appointments over the phone from the comfort of their homes while also ensuring our healthcare providers are adequately reimbursed. This vital research paper showcases the importance of telehealth services and the potential decreases in individual and taxpayer costs. Increasing awareness on the importance of telehealth services is vital, and I urge my colleagues on both sides of the aisle to support commonsense reforms, like my bill, to ensure every American has access to quality health care, regardless of where they live,” said Senator Manchin.
“Throughout the pandemic, telehealth played a crucial role in ensuring all Americans — particularly seniors and those in underserved communities — could access the health care services they needed, at no risk to themselves,” said Senator Scott. “As this report makes clear, Congress should put the lessons learned from the pandemic into action with appropriate legislation, like the CONNECT for Health Act. Doing so will not only bolster Americans’ access to quality health care today, but it will also ensure that we are better prepared for public health emergencies in the future.”
“Telehealth is a powerful tool in expanding access to quality health care across the country,” Senator Wicker said. “It is encouraging to see momentum grow in the support and utilization of such resources at both the federal and state level. I will continue to champion the permanent expansion of telehealth so that people can continue to use those services, even as we emerge from the coronavirus pandemic.”
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. with offices in Brussels and Berlin. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org and follow PPI on twitter @ppi.
Through broad-based grassroots outreach, Americans for Prosperity (AFP) is driving long-term solutions to the country’s biggest problems. AFP activists engage friends and neighbors on key issues and encourage them to take an active role in building a culture of mutual benefit, where people succeed by helping one another. AFP recruits and engages activists in all 50 states behind a common goal of advancing policies that will help people improve their lives. Learn more at americansforprosperity.org. Join us on Facebook, Twitter, LinkedIn, Instagram and YouTube.
###
Media Contact for PPI: Aaron White – awhite@ppionline.org
Media Contact for AFP: Geoff Holtzman – gholtzman@afphq.org
This report is a joint project of the Progressive Policy Institute and Americans For Prosperity.
INTRODUCTION
Prior to the COVID-19 pandemic, few Americans could access telehealth to meet their health care needs. State and national lawmakers imposed enormous obstacles on patients seeking to virtually connect with their health care provider. Policymakers feared widespread telehealth use would increase spending on unnecessary health care services. As such, Medicare banned clinicians from delivering telehealth outside of rural communities and prohibited patients from receiving telehealth within their homes.
But that dynamic changed when the coronavirus pandemic arrived in the United States, shutting down large parts of the economy and forcing families to stay home to reduce the spread of infection. In early 2020, President Donald Trump declared COVID-19 to be a public health emergency and the federal Department of Health and Human Services (HHS) used its emergency powers to temporarily suspend a variety of regulations to allow Medicare recipients to remotely access care through telehealth. In addition, states waived licensing and regulatory barriers to expand access to virtual care for individuals with commercial insurance.
As a result, telehealth became a safe, reliable source of high-quality care for tens of millions of Americans during the pandemic.
Unfortunately, without codifying these temporary reforms into law, they expire at the end of the public health emergency. The pandemic provides an opportunity to study the impact of the increasing use of telehealth services on health care outcomes and costs. Americans for Prosperity and Progressive Policy Institute worked with FAIR Health to examine how telehealth use changed during the pandemic and assess if it had an impact on costs or health outcomes improved.
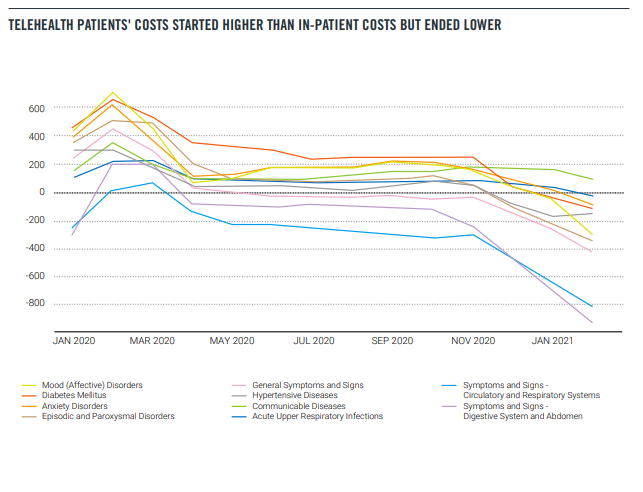
Using aggregated, de-identified data from FAIR Health, our study found that while telehealth patients’ costs started higher than in-person patients’ costs, the average telehealth patients’ health care costs fell 61%, from $1,099 per month to $425 per month between January 2020 and February 2021.
Additionally, people who used telehealth had lower overall health care utilization compared with people who used only in-person care, except during the early months of the pandemic, March to May 2020.
Our study confirms a promising trend toward cost savings for patients who use a combination of in-person and telehealth services. These results should give lawmakers confidence to extend the telehealth provisions of the public health emergency rather than letting them expire.
BACKGROUND
There is an axiom in health policy circles: “As Medicare goes, so goes the nation.” Starting in 2001, Congress authorized Medicare to deliver telehealth to the program’s recipients. However, these reforms imposed numerous restrictions that limited the availability of virtual care to a small number of seniors in rural areas. Lawmakers enacted these restrictions because they feared that making telehealth widely accessible would lead to patients accessing unnecessary services. Many clinicians were also hesitant to adopt telehealth, fearing it could disrupt existing practice arrangements and negatively affect their incomes.
But Medicare, insurers, and states shifted their telehealth policies to address COVID-19. On March 13, 2020, President Donald Trump formally declared COVID-19 a national emergency and authorized HHS to temporarily waive laws and regulations to combat and contain the virus. Several days later, Congress passed the CARES Act, which granted HHS additional powers to take emergency measures against COVID-19.
Using its new authority, HHS suspended regulations that prevented health care professionals from remotely delivering care through telehealth. The agency suspended the requirement that Medicare beneficiaries reside in a rural area to receive telehealth services. It waived restrictions that prevented patients from accessing telehealth in their home and allowed for audio-only services. In addition, it permitted rural health clinics (RHCs) and federally qualified health centers (FQHCs) to provide remote virtual care.
HHS also took groundbreaking steps to allow health professionals to deliver a greater array of remote services. The agency announced approximately 240 new telehealth services that providers can deliver to Medicare recipients, including mental health consultations and emergency care.
The agency also authorized all types of health professionals to deliver virtual care to Medicare recipients, expanding the list of telehealth-eligible practitioners to include physical therapists, occupational therapists, and speech language pathologists. Prior to COVID-19, federal law authorized only nine types of health care providers to deliver telehealth services.
Like the federal government, state governors took steps to expand the availability of telehealth to combat COVID-19. Many states suspended regulations that restricted the kinds of technologies practitioners could use to communicate with patients. Ending these restrictions allowed doctors to consult with patients through widely available technology including audio-only phone calls, online video platforms, emails, and instant messages.
Other states waived rules that limited the practice of telehealth to physicians and nurses, expanding practice eligibility to all health care providers licensed by the state. In addition, states removed many rules prohibiting patients from receiving virtual care at home.
Every state also temporarily eased or suspended costly licensing requirements to authorize health care providers licensed in other states to deliver telehealth to their residents. Prior to the pandemic, medical licensing boards charged every license applicant hundreds of dollars and forced them to wait three to nine months before they received a license to practice in their states. These reforms authorized health professionals from all over the country to support patients in pandemic hotspots.
HOW TELEHEALTH CHANGED HEALTH CARE DURING THE PANDEMIC
HHS’s emergency actions expanded access to telehealth for Medicare beneficiaries. Before the pandemic, only 134,000 Medicare enrollees received virtual care every week during the first half of 2019. After these reforms took effect, the number of enrollees receiving telehealth increased over 7,400% to 10.1 million between January and June 2020.
These reforms empowered Medicare patients to access telehealth through an array of technology options that were unavailable prior to the pandemic. Because of the availability of audio-only services, the majority (56%) of Medicare beneficiaries who used telehealth did so via phone. Roughly twice the number of Medicare beneficiaries had a telehealth visit via video (28%).
Removing state and federal barriers also expanded telehealth among individuals with commercial health plans. Prior to the public health emergency declaration in January 2020, providers delivered only 1.5% of health services through telehealth, according to claims data compiled by the COVID-19 Health Care Coalition. After these reforms took effect, providers delivered nearly 24% of all services through telehealth.
These telehealth reforms proved to be especially effective at expanding access for patients with complex conditions. Among Americans with private insurance, another study found that the majority of telehealth users used telehealth for chronic conditions, like diabetes, and behavioral conditions, including depression and anxiety. Another study found physical therapy via telehealth after hip surgery was just as clinically effective and less expensive than in-person care.
Overall, consumer interest in telehealth significantly increased during the pandemic. Prior to the pandemic, consumers were also slow to adopt telehealth. Only 11% of patients had a telehealth visit in 2019. By the height of the pandemic, utilization had increased fourfold. But while the pandemic has kickstarted a dramatic shift in health care delivery, a recent survey found that consumers are increasingly frustrated with limits on telehealth services, opaque costs, and confusing technology requirements.
Additionally, even with the expanded coverage, telehealth services are harder to access in rural areas. Rural Medicare beneficiaries reported that their health care providers were less likely to offer telehealth services than those living in urban areas (52% vs. 67%, respectively). And although telehealth seems like it could help expand the services that small rural hospitals could provide, they are the least likely to have the technology because of the upfront costs. The digital divide affects not only patients but also providers.
WHAT COMES NEXT?
These groundbreaking telehealth reforms are limited to HHS’ COVID-19 public health emergency declaration in early 2020. As soon as the secretary declares the COVID-19 crisis over, these harmful telehealth barriers will resume and patients will lose access to critical virtual care.
Medicare announced it will no longer offer payment parity for video and telephone visits after the federal public health emergency order expires. When it ends, the Medicare Payment and Access Commission (MedPAC) recommended that “Medicare should return to paying the fee schedule’s facility rate for telehealth services and collect data on the cost of providing these services.”
It also calls for ending providers’ discretion to reduce or waive cost sharing for telehealth services. MedPAC also proposed that CMS permanently establish three safeguards after the public health emergency ends to prevent unnecessary spending and potential fraud from telehealth:
Applying additional scrutiny to outlier clinicians who bill significantly more telehealth per capita
Requiring in-person visits before clinicians order expensive medical equipment or laboratory tests
Prohibiting “incident to” billing for telehealth services by clinicians who can bill Medicare
directly
Many states have already reverted to prepandemic telehealth rules. Alaska and Florida have let their public health emergency declarations expire, freezing many telehealth expansions.
However, other states, seeing the value of telehealth, have decided to let telehealth providers keep offering services over the phone pending new federal legislation enabling Medicare to reimburse for a wider spectrum of telehealth services.
TELEHEALTH LEGISLATION
Legislative action is necessary to preserve these essential telehealth reforms. To allow Medicare beneficiaries to access telehealth on a long-term basis, Senator Brian Schatz (D-Hawaii) and a bipartisan group of 59 cosponsors introduced the CONNECT For Health Act.
This bill would permanently extend COVID-era telehealth reforms and allow providers to deliver services to Medicare beneficiaries in every ZIP code in the United States, rather than just rural ones. It would also permit Medicare beneficiaries to receive virtual services from the comfort of their home and authorize important facilities such as Federally Qualified Health Centers and Rural Health Centers to deliver telehealth to patients.
Senator Joe Manchin (D-W.Va.) and other lawmakers introduced a similar bill, the Protecting Rural Telehealth Access Act, which would allow providers to offer virtual care to Medicare patients in any area of the country, permit patients to receive telehealth at home, and authorize FQHCs and RHC to provide virtual care. In addition, it would give Medicare beneficiaries the option to consult with health care providers through audio-only phone calls, video messages, and images, which proved popular during the pandemic.
Senator Tim Scott (R-S.C.) introduced the Telehealth Modernization Act to extend telehealth services to Medicare beneficiaries in any geographic area to receive virtual services, including in the home. Furthermore, it would authorize all types of health care providers to deliver virtual care to Medicare recipients. These measures would preserve the important telehealth reforms HHS implemented during the pandemic that allow providers to deliver medically appropriate virtual care.
DOES TELEHEALTH RAISE COSTS?
While many lawmakers are taking steps to permanently enact telehealth reforms into law, some fear that creating new Medicare telehealth benefits will lead to patients spending more taxpayer dollars on health care. Specifically, skeptics cite analysis from the Congressional Budget Office, which estimates removing Medicare’s telehealth limitations on virtual mental health care would increase utilization and thus spending by $1.65 billion over 10 years.
Fortunately, there is mounting evidence that telehealth can lower health care spending and reduce taxpayer costs. According to a 2021 analysis from the MedPAC, when Medicare patients chose telehealth for their primary care needs, in-person primary care visits fell by 25%.
Virtual care can also decrease health care spending by enhancing preventive care and reducing the need for patients to make expensive visits to hospitals and urgent care centers. One 2012 analysis of the Veterans Health Administration’s telehealth program for chronically ill veterans found virtual care reduced the average cost of every patient by $6,500, saving $1 billion in a single year. The program achieved these savings by reducing hospital admissions by 19% and decreasing the number of days patients spend in the hospital by 25%.
As the pandemic drags on, telehealth continues to prove it enhances patient outcomes and lowers costs. In 2020, Ascension Health found 60% of its telehealth patients would have visited an urgent care clinic or emergency room if they did not offer virtual care. This decreased outpatient visits by 33% for Ascension’s patients.
To expand on this evidence, Americans for Prosperity and the Progressive Policy Institute analyzed aggregated, de-identified data provided by FAIR Health, Inc., based on claims data from its FH NPIC® repository of privately insured medical claims. We received statistical results that reflected the experience of patients who received telehealth and those who did not have any telehealth services. The results also included a nationwide study of telehealth’s effect on patient outcomes and health care spending. Americans for Prosperity and Progressive Policy Institute studied the aggregated data results reflecting the claims experience of 8.1 million patients who used telehealth and compared them to an equivalent aggregated dataset which reflected 15.8 million patients who used inperson care only between January 1, 2020, and February 28, 2021.
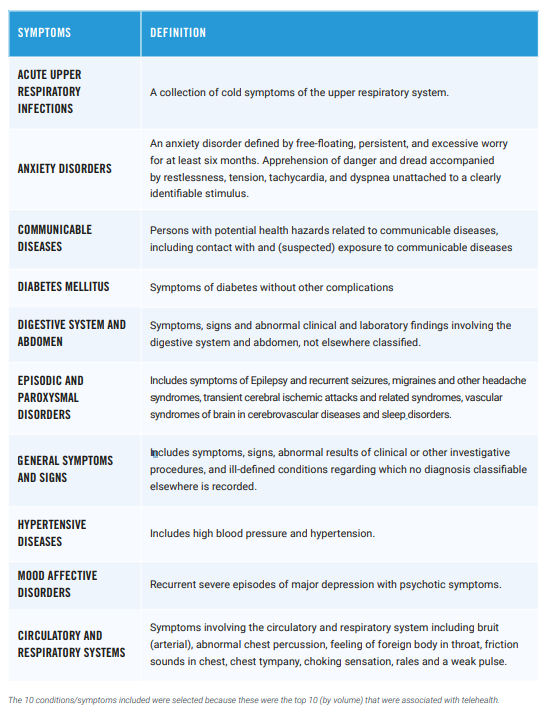
To determine telehealth’s impact on patient outcomes and costs, we compared data from FAIR Health based on de-identified patients of both groups with the same age, sex, and health conditions. The health conditions included mental disorders, hypertensive diseases, communicable diseases, respiratory infections, circulatory and respiratory symptoms, episodic and paroxysmal disorders, digestive system and abdomen symptoms, and diabetes.
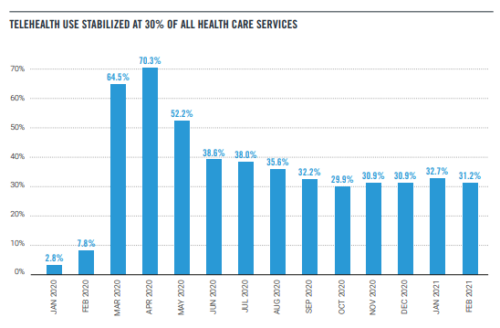
The use of telehealth skyrocketed during the early months of the pandemic. Our study found that in April 2020, telehealth appointments accounted for 70% of all health care appointments.
However, as some of normal life resumed, telehealth appointments stabilized at around 30% of all appointments. Telehealth will never fully replace in-person care, but it’s clear that it can meet patients where they are and help them access needed medical services.
TELEHEALTH PATIENTS’ COSTS
During the pandemic, patients who used telehealth spent more on health services compared with individuals who sought care exclusively from in-person providers. Over the 13-month period studied, individuals who used telehealth spent 19% more on average than in-person patients. This could be explained by the unusual care patterns during the pandemic — sicker patients may have been more afraid of catching COVID-19 and therefore tried to avoid going to the hospital by using telehealth.
Another reason could be policymakers required Medicare, Medicaid, and private health insurers to pay for telehealth services at the same reimbursement rate as in-person services, a policy known as payment parity. Lawmakers intended these measures to encourage providers to offer telehealth as more Americans sought remote care during the pandemic. However, payment parity may have artificially increased the cost of virtual care for patients and taxpayers. Without these expensive mandates, telehealth consultations can cost up to 75% less than in-person consultations. Payment parity may help explain why patients who used telehealth cost more on average than patients who didn’t.
It’s important to note, however, that patients who used telehealth spent significantly less on health services by the end of the study period compared with the start. Between January 2020 and February 2021, the average telehealth users’ monthly health care expenses fell from $1,099 to $425, a 61% decline. Telehealth patients’ costs fell faster than in-person patients: The average in-person patient spent $910 per month in January 2020 and $578 in February 2021.
The data also showed that for seven of the 10 conditions observed, patients who used telehealth spent more than patients who sought in-person care. Only telehealth patients with abdominal symptoms, respiratory symptoms, and general symptoms spent less relative to inperson patients with the same conditions. Again, this could be explained by the unusual care and payment patterns during the pandemic. However, patients of all conditions who used telehealth spent less over time. On a percentage basis, the company found individuals with diabetes, anxiety, and hypertensive diseases had a 71% reduction in spending between January 2020 and February 2021.
TELEHEALTH’S IMPACT ON UTILIZATION
Despite the increased availability of telehealth during the pandemic, for the observed conditions, utilization of the health care system did not increase for telehealth users. For seven of the 10 observed conditions, the average number of total appointments with the health care system — one way to measure utilization — was the same or fewer for people who used telehealth relative to people who did not. The only conditions where utilization was higher were anxiety disorders, mood disorders and communicable diseases. This is easily explained by the fact that anxiety and mood disorders require ongoing care and that the study period included a global pandemic and thus appointments related to communicable disease exposure were high.
In the case of emergency department visits, individuals who used telehealth accessed emergency care more often than individuals who used in-person care. During the 13-month study period, 6% of telehealth patients on average visited the ED per month. In contrast, just 3% of in-person patients accessed emergency care over this period.
But the data showed an important trend line: Individuals who used telehealth made significantly fewer emergency room visits at the end of the study period compared to the start. From January 2020 to February 2021, the average telehealth patient saw their monthly ER visit rate fall from 8.5% to 3.03%. These findings confirm prior research that found telehealth allowed providers to deliver early interventions to individuals, resulting in the use of fewer intensive services.
Taken as a whole, our findings offer strong evidence that the rise of telehealth during the pandemic has not increased overall utilization of the health care system, as many policymakers and budget hawks have feared. While some of the findings will need a longer study window to see what happens after the pandemic ends, it’s evident that consumers don’t use telehealth promiscuously. Instead, telehealth presents a promising opportunity to tailor care to individuals’ unique circumstances and makes it easier for people to access essential services.
CONCLUSION
Our analysis of the aggregated FAIR Health data shows telehealth can dramatically expand health care access without raising costs on taxpayers. Throughout the COVID-19 pandemic, state and federal officials implemented groundbreaking temporary reforms that allowed millions of Americans to remotely access essential care from qualified health professionals. As a result, many policymakers propose making long-term reforms to allow providers to deliver telehealth care on a permanent basis. However, some lawmakers fear that making telehealth available would lead to patients spending more on care by making unnecessary purchases of services.
Our analysis of FAIR Health’s data found patients who use telehealth spend significantly less on health care services over time. Between January 2020 and February 2021, the average telehealth patients’ health care expenses fell 61%, from $1,099 per month to $425 per month. Furthermore, telehealth patients purchased fewer in-person health care services such as emergency care during this time period. This suggests virtual care improves patient health and allows individuals to purchase fewer expensive procedures.
These findings hold important lessons for policymakers in Congress and around the country. Our study shows lawmakers can make important telehealth services widely available to families without raising costs on taxpayers. Therefore, Congress should permanently empower health practitioners to provide virtual care to all Medicare recipients. This would ensure seniors continue to receive quality and cost-effective care from the convenience of their homes long after the pandemic ends.
ABOUT THE AUTHORS
Arielle Kane is the director of Health Policy at the Progressive Policy Institute. Her research focuses on what comes next for health policy in order to expand access, reduce costs and improve quality.
Charlie Katebi is a health policy analyst for Americans for Prosperity, where he promotes state and federal policies that increase patient choices, lower costs, and expand access to quality health care.
By PPI’s Paul Bledsoe, Durwood Zaelke and Gabrielle Dreyfus, for the New York Times.
If the years of devastating droughts, floods, heat waves and wildfires since the Paris climate agreement was adopted have taught us anything, it’s that we have underestimated the pace of extreme, destabilizing climate change.
But delegates meeting at a world climate conference in Glasgow have more to do: For the security of the planet, they need to act further and faster to limit near-term temperature increases.
Facebook’s long-time unofficial motto was “move fast and break things.” We now see that this was a mistaken approach to building and governing a content platform. But some members of Congress who are seeking to hit back at Facebook seem to have been inspired by this same motto. Rather than taking a thoughtful approach and examining the consequences of new antitrust regulation on U.S. competitiveness and national security, the motto of these lawmakers seems to be: “Move fast, break the American tech industry and see what happens.”
We’ve tried the “move fast and break things” approach. It’s time for a new, more deliberate approach — a real effort to grapple with the benefits and harms of the tech industry and to build a regulatory framework to govern and promote the sustainable growth of American technology companies, while squarely taking on the challenge from techno-authoritarian states such as China and Russia.
What we should not do is overreact to the “Facebook Files” by passing recent bills introduced by Rep. David Cicilline (R-R.I.) and Sen. Amy Klobuchar (D-Minn.) that have nothing to do with the harms described by Facebook whistleblower Frances Haugen. These bills threaten to exacerbate those harms by creating hundreds of even less scrupulous mini-Facebooks that are beyond the reach of U.S. law enforcement and would eliminate the ability of consumers to rely on app stores to provide protection against the next social media harm.
Will Marshall, President of the Progressive Policy Institute, released the following statement in reaction to the House passage of the Biden Administration’s bipartisan infrastructure framework:
“Congratulations to Speaker Pelosi and House Democrats for passing tonight a landmark infrastructure bill that is a key pillar of President Biden’s Build Back Better agenda for an inclusive economic recovery. The president has succeeded where previous administrations have failed, and this long overdue investment in modernizing American infrastructure will create good jobs, spur economic innovation and help U.S. workers and companies outcompete China for economic and technological leadership in this century.
“It is also a rarity in Washington – a major bipartisan achievement that fulfills President Biden’s pledge to make our government work for all Americans again. The infrastructure bill enjoys broad public support, including among voters in battleground districts and states likely to determine the outcome of next year’s midterm elections.
“We were also glad to see the Progressive Caucus retreat from their counterproductive and unsuccessful strategy of holding the bill hostage to their demands for higher spending. With a second landmark accomplishment under his belt, President Biden and the party can now move on to passing a transformative Build Back Better bill that can measurably improve Americans’ lives.
“To accomplish this goal, PPI urges lawmakers to focus on delivering a few core priorities well instead of trying to enact the full progressive wish list of spending programs on a half-funded and temporary basis. We remain concerned that the House bill – as currently written – tries to do too much with too little, wastes precious resources on tax cuts for the rich, and is not offset in a sustainable way. We encourage our friends in Congress to compromise and prioritize so they can deliver a durable progressive win for the American people.”
Read PPI’s statement on the agreement to the Build Back Better framework here.
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
Twice in recent months President Biden has publicly affirmed a U.S. commitment to defend Taiwan should China attack. Both times, the White House walked his comments back, admitting that no such formal obligation exists.
While the media was quick to pounce on Biden’s “gaffes,” it’s likely that the Chinese received his message loud and clear: America has Taiwan’s back.
The United States has no mutual defense treaty with Taiwan, as we do with Japan and South Korea. On the contrary, since the 1979 Taiwan Relations Act, Washington has explicitly recognized the island as a part of China. Since then, “strategic ambiguity” has governed U.S. Taiwan policy: Washington won’t support the island’s independence so long as China refrains from seizing it by force.
The odd-year contests in Virginia and New Jersey often offer an early test of how voters think the incumbent president is doing and a foretaste of the public mood heading into the next year’s midterm elections. For Democrats, who did badly in both states last night, the message is clear: It’s time for a major course correction.
The Republican sweep of Virginia’s top offices, a year after President Biden’s 10-point victory there, was propelled by a host of factors. Former Gov. Terry McAuliffe ran a generally negative and uninspiring campaign focused mainly on trying to depict Republican Glenn Youngkin as a Donald Trump clone.
* U.S. Geological Survey reports of “apparent consumption” of steel, divided by BEA’s calculation of GDP in constant 2012 dollars. Five-year averages attempt to dampen the effects of single-year booms or crashes.
WHAT THEY MEAN:
Provisionally settling the dispute sparked by the Trump administration’s 2018 “national security” tariffs on steel and aluminum, the U.S. and European Union agreed last Saturday to a formula: 3.3 million tons of European steel products covered by the tariffs, and 18,000 tons of aluminum, will come in duty-free, with legacy tariffs of 25% and 10% still covering any additional tonnage. Official papers on this and a bit more below, but some background to the argument:
In long-term context, tariffs on aluminum tariffs were relatively new. The tariffs on steel, though using an unusual law, have a very long back-story. Analogous earlier policies, bringing analogous protest from U.S. metal-buying industries and foreign governments, date back at least to the 1970s, and range from minimum prices for imports in the Carter administration, to import quotas and “voluntary restraint agreements” in the Reagan administration, and “safeguard” tariffs in the second Bush administration. Along with these big, global, once-a-decade efforts, “trade remedy” litigation brings about a dozen anti-dumping and countervailing duty penalties per year on wire rod, welded pipe, cold-drawn alloy tube, etc., from individual countries.
What explains such a long, recurrent pattern? One obvious phenomenon, also about half a century old: the U.S. economy is getting “lighter” by using less raw materials generally, and steel use in particular hasn’t grown since the 1960s. Single-year bookends illustrate the point:
> Left bookend: In the turbulent boom-year 1968, U.S. GDP in constant dollars (using BEA’s real-GDP series) hit $4.8 trillion and employed 69 million workers. That year, Americans used 106 million tons of steel for construction projects valued at 4.4% of GDP (Lake Point Tower, the Desmond Bridge at Long Beach, the Tower of the Americas in San Antonio), finish up the Eisenhower-era National Highway System, and provide the framework for 10.8 million cars and trucks.
> Right bookend: In 2019, the constant-dollar pre-COVID economy hit $19 trillion and employed 152 million workers. It used 100 million tons of steel for construction projects valued at a slightly lower 4.2% of GDP, along with 10.9 million autos, and so on. In COVID-stricken 2020, use dropped to 82 million tons.
More systematically, since the late 1960s U.S. steel use has remained flat in total tonnage, and relative to economic output has dropped by about 75%. The totals look like this, using five-year averages to avoid distortions by 1968-like booms or 2020-like busts: an average of 95 million tons of steel per year from 1968-1972, in a real-GDP U.S. economy of about $5 trillion; 98 million tons from 1993-1997, in an economy that had doubled in real terms to $10 trillion; and again 95 million tons a year in 2016-2020, for an economy of $18.4 trillion. Or, relative to real-dollar output, a half-century ago $1 billion of constant-dollar GDP meant orders for 18,850 tons of steel; in the mid-1990s it meant 9,200 tons; today, it means 5,400 tons.
In such circumstances, absent a structural solution in new demand at home or abroad — the logical candidate just now is larger long-term public infrastructure investment — any increase in imports feels like it’s coming at the expense of local production. Hence, presumably, the constant return to import limits.
FURTHER READING
USTR and the Department of Commerce announce a U.S.-EU agreement, with details and quota numbers in the links at bottom of this section.
Why would steel use fall? It is tempting, but at minimum not the whole answer, to say that the use of import restrictions is itself part of the reason. The logic would be that minimum import prices, VRAs, safeguards, 232 tariffs, etc. push up steel prices, upset ‘downstream’ industries like construction firms and machinery makers, and when sustained over time convince them to substitute other materials. But if so, we’d expect use of other metals and materials to rise as steel use drops. In fact, though, U.S. use of other metals — and raw materials in general — is also flat in absolute terms and down relative to output. Relative to constant-dollar GDP, lead use is down by about 66%, cement by 60%, copper 75%, crushed stone 50%, crude oil by 66%, and tin more than 80%. So if import limits haven’t been solutions, they also don’t look like the main problem.
Instead, the U.S. economy as a whole has become steadily ‘lighter’: in aggregate, the GDP shares of information, professional and business services, health, arts, and education have risen from 13.1% of GDP in 1970 to 22.1% in 1995 and 27.9% in 2020; simultaneously, the GDP shares of big metals-buyers in durable-goods manufacturing and construction have dropped from 18.3%in 1970 to 13.3% in 1995 and 10.2% in 2020.
The U.S. Geological Survey reports on production, imports, consumption, etc. of 124 metals and minerals from 1900 forward (use “Mineral Commodity Summaries” for 2016-2020 data), which can be found here.
USITC’s list of anti-dumping and countervailing duties in force can be found here.
The World Steel Association has production data in detail from 2002 forward, found here.
For perspective, a 1984 National Bureau of Economic Research report on steel import limits can be found here.
ABOUT ED
Ed Gresser is Vice President and Director for Trade and Global Markets at PPI.
Ed returns to PPI after working for the think tank from 2001-2011. He most recently served as the Assistant U.S. Trade Representative for Trade Policy and Economics at the Office of the United States Trade Representative (USTR). In this position, he led USTR’s economic research unit from 2015-2021, and chaired the 21-agency Trade Policy Staff Committee.
Ed began his career on Capitol Hill before serving USTR as Policy Advisor to USTR Charlene Barshefsky from 1998 to 2001. He then led PPI’s Trade and Global Markets Project from 2001 to 2011. After PPI, he co-founded and directed the independent think tank ProgressiveEconomy until rejoining USTR in 2015. In 2013, the Washington International Trade Association presented him with its Lighthouse Award, awarded annually to an individual or group for significant contributions to trade policy.
Ed is the author of Freedom from Want: American Liberalism and the Global Economy (2007). He has published in a variety of journals and newspapers, and his research has been cited by leading academics and international organizations including the WTO, World Bank, and International Monetary Fund. He is a graduate of Stanford University and holds a Master’s Degree in International Affairs from Columbia Universities and a certificate from the Averell Harriman Institute for Advanced Study of the Soviet Union.
The death of the American middle class has been a potent theme in political discourse and on the pages of mainstream publications for decades. Good jobs for “middle-skill” workers were pulled down by the implosion of manufacturing employment, on the one hand, and the growth of the poorly paid and perpetually-squeezed health care sector, on the other. The classic “steelworker to nurse or health technician” story ends up requiring much more education for the roughly the same pay. Steel production workers earn an average of $23 per hour, according to BLS figures, while licensed practical and vocational nurses, which require at least a year of extra education, earn an average of $24 per hour.
But for those pundits searching for the new middle class, there is good news. The tech-ecommerce boom has become the biggest source of “good jobs” both nationally and in most states. Since September 2017 to September 2021, the tech-ecommerce ecosystem — composed of thousands of small and large firms in addition to the big tech companies — created 1.4 million jobs in the United States. That’s three times as many as health care, the previous champ of job creation, which added 500,000 jobs over that same stretch. The rest of the economy lost 900,000 jobs.
This stunning job growth, surprisingly underappreciated and even mocked by many progressives, is building a new middle class across the United States. The key is that tech and e-commerce companies pay “middle-skill” Americans a better wage than they can get at other employers, including hospitals and senior citizen facilities. Our analysis of government data shows that workers with some college, including an associate’s degree, earn 32% more in tech-ecommerce than in the economy as a whole. Average pay in tech-ecommerce — including all positions from coders to fulfillment center workers — varies from state to state, but it is higher than average pay in manufacturing in 42 states, and higher than average pay in health care in every state.
This central role of tech-ecommerce in generating well-paid middle-skill jobs is new. During the 1990s tech boom, which I wrote about extensively as economics editor and then chief economist at BusinessWeek, the great majority of new tech jobs required a college education. Software developer jobs in Silicon Valley were not a viable replacement for the manufacturing middle class.
But today, tech-ecommerce firms are creating a broader array of jobs. As of 2019, tech-ecommerce companies employed 1.8 million American workers with some college, in occupations like computer support specialists and network and computer system administrators. (That figure is based on our tabulations of the March 2020 Annual Social and Economic Supplement to the Current Population Survey, covering 2019 earnings and employment). The higher pay and job creation is being fueled by huge productivity gains in the tech-ecommerce sector, which are being passed onto workers, just as economic theory would predict.
Here’s where the growth of the new tech-ecommerce middle class intersects with policy. Although I have always been an avid supporter of tech-driven growth, tech has never been the unalloyed panacea that many in the industry claimed. In 2000 I wrote a book entitled “The Coming Internet Depression,” that emphasized the volatility of tech jobs. More recently, it’s become clear that the tech-ecommerce ecosystem would benefit from more regulation.
But not all forms of regulation are created equal. The most radical of the antitrust bills now being considered by Congress, including the new legislation sponsored by Senator Amy Klobuchar (D-Minn.), titled “The American Innovation and Choice Online Act,” are specifically designed to change the way that big tech companies do business, and to protect less efficient competitors.
Tech critics are engaged in the equivalent of ripping random parts out of a smoothly running car engine, while assuring the passengers — American workers, in this case — that the parts aren’t necessary and that the car still runs just as fast.
Some have accused Big Tech of engaging in labor market “monopsony,” meaning that they control the demand side of job markets. But if tech firms were behaving like labor market monopsonists, they would be holding down hiring and wages. That’s so clearly not happening, it’s laughable. Between 2012 and today, the five big tech firms went from 300,000 to almost 1.9 million workers globally, in perhaps the biggest surge of “good job” hiring in recorded history. Other tech company employment grew as well. Salesforce went from 8,000 workers to 56,000. Cognizant, an IT consulting firm with a large global footprint, went from 27,000 U.S. workers to 44,000.
In September, Amazon announced plans to hire 125,000 new workers, at an average starting pay of $18 per hour, which translates into $36,000 per year for full-time work, without counting overtime or bonuses. To put that in perspective, two parents starting at an Amazon fulfillment center would earn $72,000 per year together, roughly comparable to the $68,000 median household income reported by the Census Bureau.
What’s happening is that tech-ecommerce is filling the middle-skill job hole in the economy that health care failed to fill. Health care is a low-productivity industry which overworks and underpays its employees, as you might expect given its highly regulated nature. The average pay for tech-ecommerce workers with some college (including an associate’s degree) is roughly $59,000, compared to $41,000 for people with a similar education in the health care and social assistance sector. The average pay for tech-ecommerce workers with a high school diploma is $42,000, compared to $31,000 for people with a similar education in the health care and social assistance sector. To put it by occupation, health technologists and technicians get paid a median hourly wage of $21.93, while computer support specialists get paid a substantially higher wage of $26.69.
What about manufacturing? Let’s consider Eastman Kodak, a “progressive” company featured by Rick Wartzman of the Drucker Institute in his 2017 book on the “good jobs” of the past. Kodak, which employed 145,000 workers globally at its peak paid its workers well above the national average and provided a fleet of benefits. Kodak’s founder, George Eastman, introduced a form of profit sharing — the so-called wage dividend — in 1912. In the 20 years from 1959 to 1979, Kodak’s workforce doubled in size, and real average pay for employees doubled as well.
Kodak’s ability to sustain well-paying jobs for its workers was closely linked to its willingness to invest in new technology. Kodak pursued an active research agenda, patenting new inventions that kept it ahead of rivals and potential entrants. “By the time rivals found ways around the current technology,” wrote one study from the Brookings Institution, “Kodak was on to the next technology.” One surprising example: Kodak was the original company behind Super Glue, which it later licensed.
Despite decades of antitrust actions and consent degrees, Kodak still controlled 80% of the amateur photographic film market in 1979. According to researcher Kamal Munir of Cambridge Judge Business School, “gross margins on film ran close to 70%, and its success was further underpinned by a massive distribution network and one of the strongest brands in the world.”
Would workers have been even better off if Kodak had been broken up for antitrust reasons? One could debate that question endlessly. But one thing is clear: Production workers at Kodak benefited from being part of a large company that excelled at R&D and marketing, and that actually manufactured products in the United States. That helped create good jobs.
Conversely, business strategies that separate out production from R&D and product development have proved to be a disaster for less educated workers, who fare better when they are part of the “mother ship” and entitled to the same benefits and pay structure as their highly educated counterparts.
That’s what makes the progressive attack on tech the ultimate self-destructive act politically and economically. They are undercutting the very middle-income workers that progressives claim to care about.
No one denies that Big Tech merits closer regulatory attention. But we have to remember that progressive historically has two meanings. One strand is the fight against corporate corruption, which is essential to keep capitalism on the rails. The other strand is about economic progress and raising living standards. We have to balance the two.
The Build Back Better Framework released by the White House on Oct. 28 would make some potentially transformative investments in American society. But those investments are severely weakened because most are scheduled to expire after only a few years to make the 10-year cost of the bill seem smaller than it really is. Advocates of this tactic hope that these temporary programs will prove so popular that a future Congress will extend them. But this risky bet would make it easier for a Republican-controlled Congress to kill the Democrats’ accomplishments without actually addressing the concerns of their fiscally pragmatic members.
While today’s lawmakers may like their own proposals, they cannot be sure that a future Congress will continue funding programs that are scheduled to expire. Making the Democratic agenda temporary empowers Republicans who want to repeal it.
Will Marshall, President of the Progressive Policy Institute, released the following statement in reaction to President Biden’s announcement of a deal on the Build Back Better framework and imminent vote on the bipartisan infrastructure package:
“President Biden today unveiled a revised Build Back Better framework that better reflects his party’s diverse coalition, and he urged Democratic lawmakers to proceed to a vote on his bipartisan infrastructure bill.
“PPI applauds the president’s diligent efforts to forge a new consensus behind a more balanced and realistic reconciliation bill. While we are concerned that the new framework tries to do too much with too little, we believe all progressives need to compromise to help President Biden deliver on his core commitments to working Americans.
“We call on the House Progressive Caucus to stop threatening to vote down the president’s infrastructure bill. They have been heard for months and many of their demands have found their way into the new framework.
“The new $1.8 trillion framework in important respects resembles one PPI published earlier this month as a pragmatic alternative to the left’s $3.5 trillion wish list. Our package cost just under $2 trillion, with roughly half the money focused on helping working families, one third on combatting climate change and the remainder being used to cover the uninsured and lower premiums for those with health insurance.
“Unfortunately, many of these core priorities are cut short because the new White House framework tries to enact too many programs on a temporary basis instead of prioritizing a few robust and transformative initiatives. We think many of these programs merit further study and deliberation and that they should be taken up in subsequent legislation rather than depriving core initiatives of permanent funding in the current bill. We also have serious concerns about whether the tax policies included in the framework will actually produce enough revenue to fully pay for the spending, particularly if all these ostensibly temporary programs are eventually extended or made permanent.
“As the framework is translated into legislative language, we hope to see further refinements aimed at allaying such concerns. In the meantime, we commend President Biden for patiently brokering the compromises necessary to get his Build Back Better bills across the finish line. Together with the American Rescue Plan, they would have a transformative impact on American jobs, innovation and competitiveness, and would ensure a more inclusive economic recovery that helps those hit hardest by the pandemic.
“It’s past time to stop debating and take the first step by passing the bipartisan infrastructure bill.”
Earlier this month, the Progressive Policy Institute released a focused blueprint for delivering on President Biden’s promise to Build Back Better while addressing the concerns of moderates who cannot support $3.5 trillion of new spending. The report, titled “Reconciling with Reality: The top priorities for building back better,”outlines a bold plan to deliver on three urgent priorities of the Democratic party within the confines of a roughly $2 trillion bill: supporting working families, combating climate change, and expanding access to affordable health care for those in need. Read it here.
The Progressive Policy Institute (PPI) is a catalyst for policy innovation and political reform based in Washington, D.C. Its mission is to create radically pragmatic ideas for moving America beyond ideological and partisan deadlock. Learn more about PPI by visiting progressivepolicy.org.
FACT: The U.S. trade deficit is up ~60% since 2016.
THE NUMBERS:
$1.05 trillion*: U.S. manufacturing trade deficit, 2021 $0.90 trillion: U.S. manufacturing trade deficit, 2020 $0.65 billion: U.S. manufacturing trade deficit, 2016
* Educated guesswork for a volatile post-COVID closure period, based on 8 months of available data for 2021
WHAT THEY MEAN:
Each February, the Office of the U.S. Trade Representative puts out a report entitled “The President’s Trade Agenda,” meant to set out administration goals for the coming year. The 2017 edition, the first of the Trump administration, cited U.S. trade balance statistics as proof that early administrations got things wrong: “In 2000, the U.S. trade deficit in manufactured goods was $317 billion. Last year it was $648 billion — an increase of 100%.” The next one, in 2018, used “bilateral” trade balance to (a) claim failure for the North American Free Trade Agreement (“our goods trade balance with Mexico, until 1994 characterized by reciprocal trade flows, almost immediately soured after NAFTA implementation, with a deficit of over $15 billion in 1995, and over $71 billion by 2017”) and (b) define a goal for a renegotiated “USMCA”: “USTR has set as its primary objective for these renegotiations to improve the U.S. trade balance and reduce the trade deficit with the NAFTA countries.”
Few economists see trade balance as a useful way to judge trade policy, whether in terms of the content of agreements, or the nature of permanent systems like tariff schedules and antidumping laws. In the standard Econ 101 equations, a country’s trade balance will always match the difference between its savings and its investment; since the mid-1970s, Americans have been investing more than we save; ergo, deficits result. In this view, very high deficits can cause alarm as indicators of unsustainable booms and potential financial shocks, but the appropriate response is long-term measures to raise savings rates. Trade policy, meanwhile, should be judged against hopes for growth, job quality, control of inflation, raising living standards for low-income families, business competitiveness and innovation, and so on.
But shoving such high-minded quibbling aside, how do the Trump legacy policies — tariffs on metals and Chinese goods, withdrawal from the World Trade Organization’s Dispute Settlement Body, the new USMCA, etc. — look when judged by the standards the 2017 and 2018 reports set?
1. By 2020, the U.S. deficit in manufactured goods had hit $900 billion. This is a four-year jump of $252 billion, not much below the $331 billion 16-year increase cited in the 2017 report. Barring some unexpected economic shock this November, the 2021 figure will easily top $1 trillion.
With respect to Mexico specifically, the bilateral goods deficit in 2020 was $114 billion. The 2021 figure looks about the same. Adding Canada gets a total north of $150 billion.So by these standards, not too good. Not what the policies’ authors predicted. And some grounds for high-minded quibblers to smirk.
Trumpism leaves a larger deficit overall, and more concentrated in manufacturing than the 2016 figures. The basic figures are, pulling the lens steadily back:
(a) The U.S. “goods” deficit — exports of manufacturing, energy, agriculture, scrap and waste and uncategorized small-scale shipments minus the equivalent imports — was $749 billion in 2016 and $922 billion in 2020. The manufacturing deficit was equivalent to 86% of the 2016 total, and by 2020 had risen to 98% of the total. A 2021 annualization suggests a total goods deficit around $1.05 trillion in 2021, with manufacturing more than 100% of the total and other goods in small net surplus.
(b) A broader measure, counting services trade (generally in surplus for the United States) as well as goods, finds a goods/services trade deficit up from $481 billion in 2016 to $677 billion in 2020. The 2021 figure is likely to be around $900 billion.
(c) Relative to GDP (more meaningful), a deficit of 2.7% of GDP in 2016 rose to 3.1% in 2020, and a likely 4% in 2021. This would be the highest since the modern-era peaks of 5.7% in 2005 and 2006.
Why the jump? Tax policy is the obvious suspect. Three of the four upward ratchets in U.S. trade deficits since the 1970s followed tax-cut bills — one in the first Reagan term, another in the second Bush administration, and the third in 2017. Bills of this sort bring higher government deficits. Unless a rise in family or business savings offsets this public dis-savings, overall U.S. savings will fall, and all else equal, by virtue of the “savings – investment = trade balance” identity, trade deficits rise. So the higher 2020 and 2021 deficits likely emerge from the 2017 tax bill.
The Trump-era tariffs likely had relatively little trade-balance impact, but do seem to have had two outcomes. One is a shift in import patterns: imports from China, though slightly above 2016 levels in dollar terms, have dropped from 21.6% of goods imports to 18.1% in 2020 and 2021, as clothes, consumer electronics, etc. from Vietnam, India, Taiwan, and so forth replace some Chinese-origin goods. Second, some shift in composition, with relatively more manufacturing deficits and relatively less energy. Where the permanent U.S. tariff system is mostly a way to tax clothing and shoes and so falls mainly on retailers and families, Trump-era tariffs on steel, aluminum, and Chinese goods were more concentrated in industrial inputs such as metals, auto parts, electrical converters, etc. As an example, tariff revenue on insulated electric conductors rose from $56 million in 2017 to $322 million in 2020. As U.S. manufacturers absorb these costs, the likely result is marginal loss of competitiveness both for exporters trying to sell to foreign buyers and for firms competing against imports at home (and of course exporters facing retaliation by foreign countries responding to tariffs), pushing more of the U.S deficit into manufacturing.
… and also read the 2018 follow-up (with a wildly wrong claim that the 2017 tax bill “has the potential to reduce the U.S. trade deficit by reducing artificial profit shifting”).
And so … “House on fire! Bring more kerosene!” In the Economist last month, Trump-era lead trade negotiator Robert Lighthizer again laments high trade deficit, skates around the 2017-2021 rise, and suggests more of the 2018-2020 approach will bring it down this time. Read the Economist piece here.
There is a massive amount of wasteful spending in healthcare. Credible research suggests that roughly one-quarter of our total healthcare spending is wasted on low-value care, administrative complexity, including prior authorization processing, and failure of care delivery.
However, there is at least one area in healthcare that is indisputably high value: vaccines. Vaccines are widely regarded as the most cost-beneficial intervention in healthcare. Unfortunately, and counterintuitively, current cost-sharing policies discourage our most vulnerable population – seniors – from accessing vaccines.
Most private insurance policies or Affordable Care Act (ACA) plans provide coverage for vaccines without any out-of-pocket cost to the patient to encourage patients to be vaccinated. Regrettably, the same cannot be said for Medicare. Medicare coverage of vaccines for seniors is a tale of two cities. Vaccines paid for through Medicare Part B that are recommended by the Advisory Committee on Immunization Practices (ACIP) require zero out-of-pocket costs for patients. However, newer vaccines recommended by ACIP, except those for COVID-19, are covered under the Medicare Part D benefit and require an out-of-pocket expense for the beneficiary that can range from a few dollars to the entire cost of the vaccine.